
Infographics – Recommendations for Hydroxychloroquine & Chloroquine Toxicity
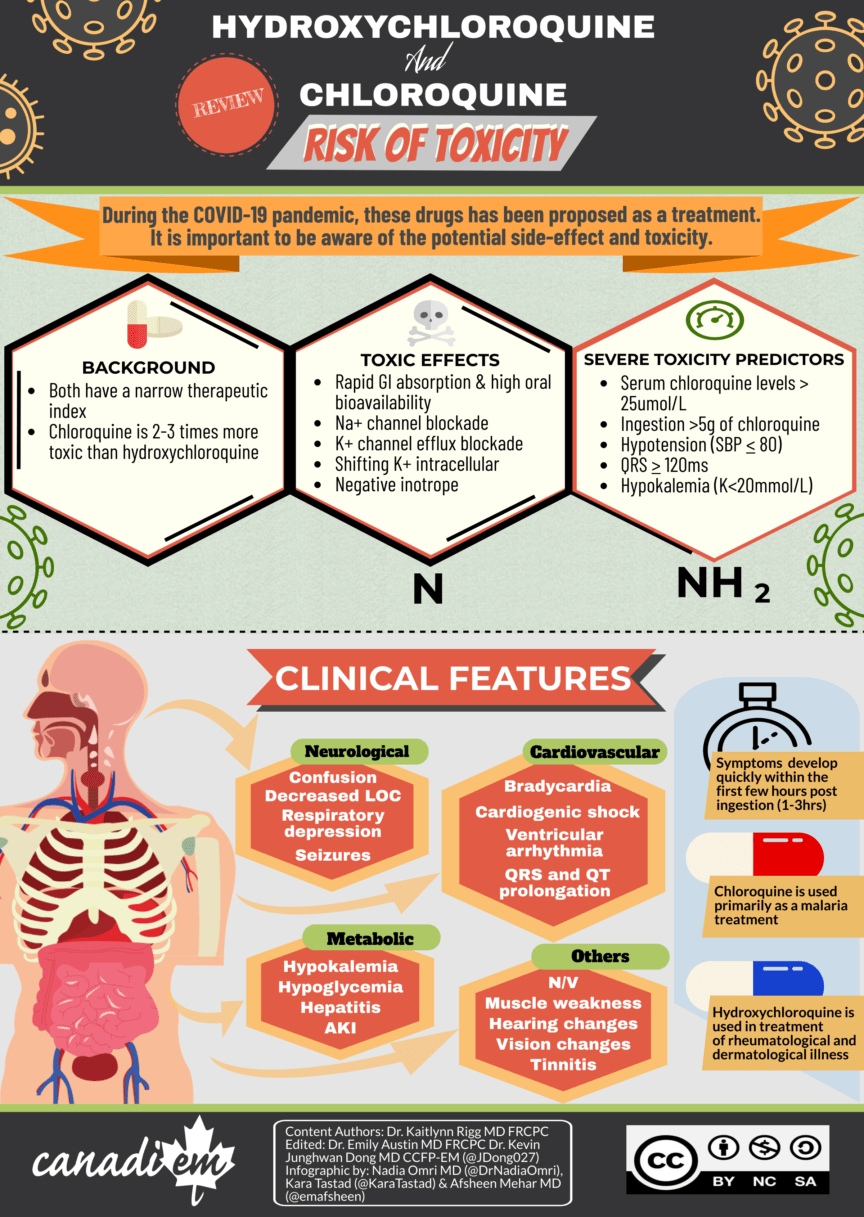
During the COVID-19 pandemic, there have been many attempts to find treatments for the virus. One of the main medications proposed for treatment and very prominent in the media has been the use of chloroquine and hydroxychloroquine. As many research studies are under way to evaluate the efficacy of this drug, we currently do not have robust evidence for positive clinical outcomes. However, there have been reports of individuals using these medications without the appreciation for potential toxic side effects resulting in accidental overdose and even death.
In this article, Dr. Kaitlynn Rigg, who is a board-licensed Emergency Medicine Physician and Toxicologist, reviews the hydroxychloroquine/chloroquine toxicity and how we can treat patients, who present with potential overdose.
[bg_faq_start]BACKGROUND
- Class of 4-aminoquinolines
- Chloroquine discovered first, hydroxychloroquine synthesized later as b – hydroxylated derivative
- Chloroquine is used primarily as a malaria treatment whereas hydroxychloroquine is used in various rheum and derm conditions such as SLE and RA due anti-inflammatory effects and better tolerability.
- Both drugs have a narrow therapeutic index where toxicity can be seen with doses just outside the therapeutic range
- Chloroquine appears to be 2-3 times more toxic than hydroxychloroquine
TOXIC EFFECTS
A variety of toxic effects can be seen with hydroxychloroquine/chloroquine toxicity, these include:
- Rapid GI absorption with high oral bioavailability
- Na channel blockade
- K channel efflux blockade
- Shifting K intracellular
- Negative inotrope
- Other toxic features: Methemoglobinemia (rare), hypoglycemia, hepatitis, myopathy, neuropathies, SNHL, direct retinal toxicity (chronic use)
PREDICTORS OF SEVERE TOXICITY
When determining the severity of hydroxychloroquine/chloroquine toxicity, the following are often predictors of severe toxicity:
- Ingestion > 5g of chloroquine
- QRS > 120ms
- Hypotension (SBP < 80)
- Degree of hypokalemia (K <2mmol/L)
- Serum chloroquine levels > 25umol/L
- Early spontaneous vomiting likely protective (self-decontamination)
CLINICAL FEATURES
Symptoms of hydroxychloroquine/chloroquine toxicity develop quickly within the first few hours post ingestions (1-3hrs). Significant ingestions can show rapid progression to coma and cardiovascular collapse in this timeframe. Main systems involved in these clinical features include:
- Cardiac:
- Cardiogenic shock, ventricular arrhythmias, QRS prolongation, bradycardia
- QT prolongation, Torsades de Pointes
- CNS
- Decreased LOC, confusion, seizures, respiratory depression
- Metabolic
- Profound hypokalemia secondary to intracellular shift. This resolves after acute toxicity improves and rebound hyperkalemia can occur if potassium replacement is overly aggressive.
- Hypoglycemia
- Hepatitis
- Acute Kidney Injury
- Others: Early Nausea/Vomiting, hearing changes/ tinnitus, vision changes, muscle weakness
TREATMENT
When initiating treatment, always call your local poison center early for guidance! Keep in mind that severe toxicity usually improves after 24hrs.
Decontamination:
- Gastric lavage may be considered if there is an early presentation post-ingestion (<1hour) with a significant amount of ingestion, and the provider is comfortable with the procedure.
- Activated charcoal is appropriate if presentation is <2hrs after ingestion and after intubation for airway protection. Remember moderate to severely poisoned patients can decline precipitously, thus charcoal should be administered only AFTER airway protection to avoid risk of charcoal aspiration. Remember, these drugs bind charcoal really well and could be considered later post ingestion under poison center guidance.
- There is no role for dialysis due to high volume of distribution and significant protein binding.
Shock
- Early Intubation – for anticipated rapid clinical decline in severely poisoned patients
- IVF Bolus
- Early initiation of epinephrine infusion – begin at 0.25mcg/kg/min and titrate to effect. Epinephrine is proposed as vasopressor of choice due to additional inotropy benefit. There is evidence of bundle therapy of epinephrine plus diazepam in chloroquine poisoned patients that shows mortality benefit.
- High dose diazepam – begin at 2mg/kg IV over 30 minutes followed by 1-2kg/kg per day for 2-4 days. Demonstrates a potential mortality benefit for severely poisoned patients. The mechanism is unclear, though diazepam may be a specific cardiac antagonist of chloroquine. Other studies of more moderately poisoned patients did not show benefit.
- Addition of other vasopressors/ inotropes (norepinephrine/dobutamine) as needed given response to therapy
QRS widening
- Sodium bicarbonate – Boluses 1-2 amps IV. May worsen hypokalemia and risk of QT prolongation; therefore, wait for a potassium level before administering. If potassium unknown or QT significantly prolonged consider 3% saline instead.
- 3% saline – 1-2mL/kg IV bolus
QT prolongation & hypokalemia
- K replacement if significant hypokalemia/ arrhythmias but watch for rebound hyperkalemia as this is due to shift of intracellular K rather than total body depletion.
- Other options include: Mg sulphate 2-4g IV or Isoproterenol for extremely refractory QT prolongation.
- Torsades de Pointes is treated in the normal fashion (ex. cardioversion/ defib, overdrive pacing both chemical or electrical).
Ventricular Arrhythmias (VT/VF)
- Use cardioversion as needed and Lidocaine if refractory. Avoid amiodarone due to the risk of QT prolongation!
Seizures
- Benzodiazepines are first line treatment for seizures due to chloroquine and hydroxychloroquine toxicity.
Arrest or deteriorating patient?
In deteriorating patients intralipid could be considered based on the drugs lipophilicity (log P 4.3) but little evidence exists to support its benefit. ECMO may be a better option if available as patients can survive neurologically intact if supported through the cardiogenic shock phase
[bg_faq_end][bg_faq_start]TREATMENT INFOGRAPHIC

DISPOSITION
Assessment and observation is recommended for chloroquine and hydroxychloroquine ingestions that fall outside of the normal therapeutic dosing range (due to narrow therapeutic index) or if:
- Patients are symptomatic, intentional ingestions or under the guidance of local poison center
- Be cautious with peds patients as even 1-2 pills can be extremely toxic if ingested so have a lower threshold for observation
Consult ICU for support if moderate to severe ingestion given high risk for rapid and precipitous for deterioration.
Always remember to screen for mental health and suicide risk in any patient presenting with overdose or toxicity.
[bg_faq_end][bg_faq_start]REFERENCES
Bagate F, Radu C, Mekontso Dessap A, de Prost N. Early extracorporeal membrane oxygenation for cardiovascular failure in a patient with massive chloroquine poisoning. Am J Emerg Med. 2017; 35:380.e3-380.34.
Barry J. Antimalarials. In: Hoffman R, Howland M, Lewin M, Nelson L, Goldfrank L, eds. Goldfrank’s Toxicologic Emergencies. 10th Ed. New York: McGraw-Hill Education; 2015:800-811.
Clemessy JL, Angel G, Borron S, et al. Therapeutic trial of diazepam versus placebo in acute chloroquine intoxications of moderate gravity. Intensive Care Med. 1996; 22:1400-1405.
Clemessy JL, Taboulet P, Hoffman J, et al. Treatment of acute chloroquine poisoning: A 5-year experience. Crit Care Med. 1996; 24:1189-1195.
Cole J, Stellpflug S, Smith S. Refractory hypotension and ventricular fibrillation with large U waves after overdose. JAMA Intern Med. 2016; 176:1007-1009.
De Olano J, Howland M, Su M, et al. Toxicokinetics of hydroxychloroquine following a massive overdose. Am J Emerg Med. 2019; 37:2264.e5-2264.e8.
Haesendonck R, de Winter S, Verelst S, Sabbe M. Intravenous lipid emulsion for intentional chloroquine poisoning. Clin Tox. 2012; 50:223-223.
Neuvonen P, Kivisto K, Laine K, Pyykko K. Prevention of chloroquine absorption by activated charcoal. Hum Exp Toxicol. 1992; 11:117-120.
Reuters T. (2020, March 24). Arizona man dead, wife in hospital after ingesting chloroquine over coronavirus fears. CBC. https://www.cbc.ca/news/world/arizona-chloroquine-death-1.5507775
Riou B, Barriot P, Rimailho A, Baud F. Treatment of severe chloroquine poisoning. N Engl J Med. 1988; 318:1-6.
Smith E, Klein-Schwartz W. Are 1-2 dangerous? Chloroquine and hydroxychloroquine exposure in toddlers. J Emerg Med. 2005; 28:437-443.
White N. Cardiotoxicity of antimalarial drugs. Lancet Infect Dis. 2007; 7:549-558.
Wong A, Cheung I, Graham C. Hydroxychloroquine overdose: case report and recommendations for management. Eur J Emerg Med. 2008; 15:16-18.
York G. (2020, March 22). Nigerians poisoned after taking doses of drug praised by Trump. The Globe and Mail. https://www.theglobeandmail.com/world/article-at-least-two-cases-of-chloroquine-poisoning-in-nigeria-after-trump/
[bg_faq_end]This post was peer-reviewed and edited by Dr. Emily Austin MD FRCPC. It was edited by Dr. Kevin Junghwan Dong MD CCFP-EM and Kara Tastad.

Kaitlynn Rigg
Latest posts by Kaitlynn Rigg (see all)
- Hydroxychloroquine & Chloroquine Toxicity Review - April 14, 2020

Emily Austin
Latest posts by Emily Austin (see all)
- Hyperthermia in Methamphetamine Toxicity - January 18, 2022
- Queen’s Gambit Case Report: Pediatric Benzodiazepine Overdose - March 18, 2021
- Hydroxychloroquine & Chloroquine Toxicity Review - April 14, 2020

Kevin Junghwan Dong
Latest posts by Kevin Junghwan Dong (see all)
- Methoxyflurane- an alternative to opioid and NSAID analgesia in the Emergency Department? - July 8, 2021
- The CAEP Daily: Day 2 (June 16) - June 16, 2021
- CAEP 2021: Recent EM Literature and Global EM Tracks - June 10, 2021