
Is first pass success without hypoxemia increased with the use of apneic oxygenation during rapid sequence intubation in the emergency department?
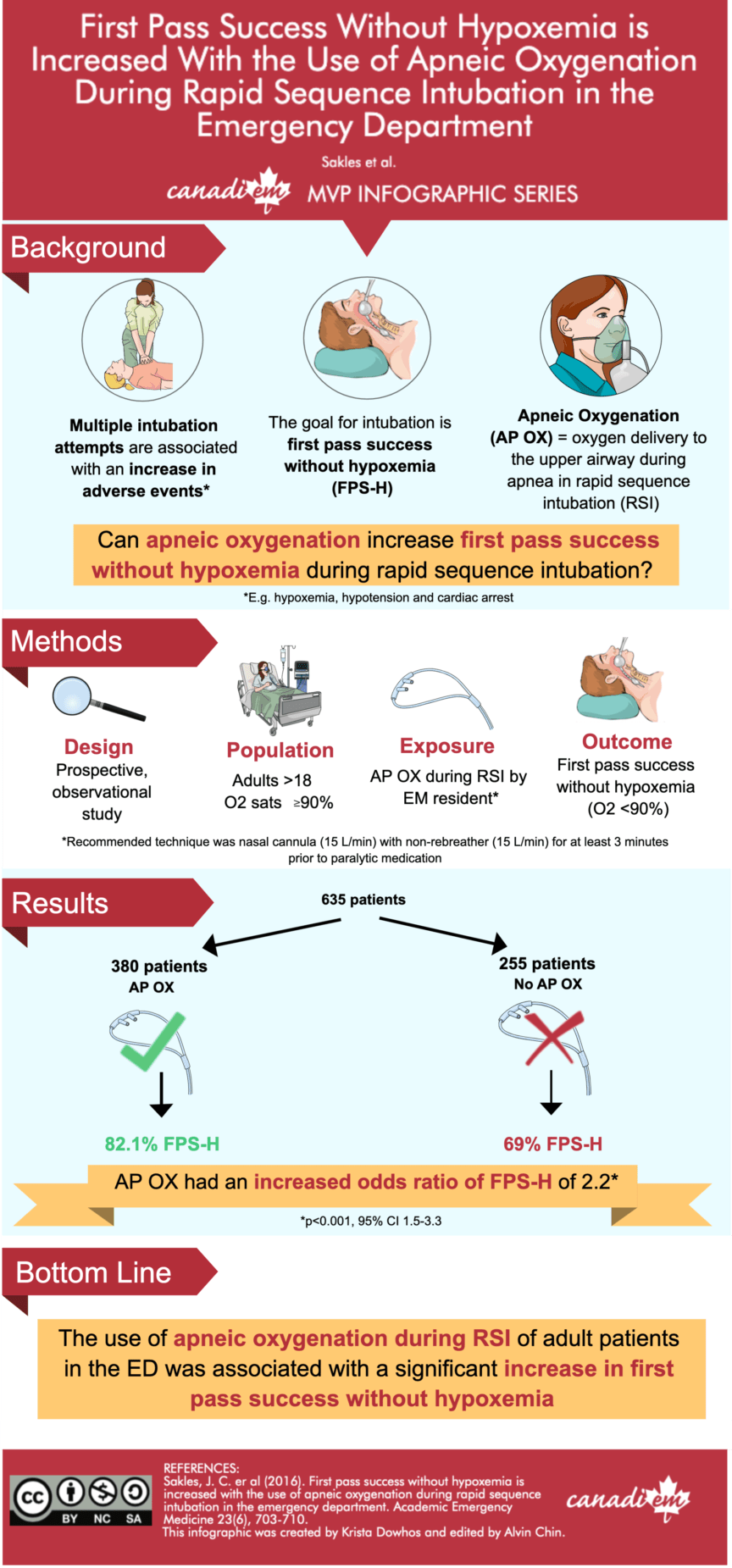
As part of the MVP infographic series, this post reviews an article by Sakles et al. looking at apneic oxygenation in rapid sequence intubation (RSI). Previous studies have shown that multiple intubation attempts during RSI are associated with an increase in adverse events such as hypoxemia, hypotension, and cardiac arrest1–6. Thus, it should be the goal of the emergency provider to obtain First Pass Success Without Hypoxemia (FPS-H) during tracheal intubation7. Apneic oxygenation (AP OX) is the delivery of oxygen to the upper airway during RSI when the patient is apneic. Previous studies suggest that apneic oxygenation is associated with a delay in oxygen desaturation during tracheal intubation. However, these studies were done in controlled environments such as the operating room, where patients were not critically ill8–13.
Sakles et al. performed a single centre, prospective, observational trial to determine if AP OX would be associated with FPS-H during RSI performed by emergency medicine residents in the ED8. They studied adults >18 years of age undergoing RSI, who had an initial oxygenation saturation of greater or equal to 90%. The exposure was AP OX during RSI, and EM residents were strongly encouraged to adopt this method during the study period. The recommended technique was to place a nasal cannula at an oxygen flow rate of 15 L/min underneath a nonrebreather facemask at 15 L/min during pre-oxygenation. Then, after the patient was rendered apneic, they would leave the nasal cannula in place and allow it to provide AP OX during laryngoscopy. The primary outcome for this study was FPS-H.
In the AP OX cohort , FPS-H was 312/380 (82.1%) and in the no AP OX cohort FPS-H was 176/255 (69.0%; difference = 13.1%; 95% confidence interval [CI] = 6.2% to 19.9%). AP OX had an increased odds ratio of FPS-H of 2.2 (p<0.001, 95% CI 1.5-3.3).
The authors’ conclusion was that first pass success without hypoxemia was increased with the use of apneic oxygenation during RSI in the emergency department.
Study Limitations
There were several limitations to this study. First, the two cohorts studied were not balanced. The AP OX cohort had less trauma patients and less difficult airways. This could have biased the results to make AP OX appear to be more beneficial than it truly was. Second, patients were only included if they were intubated by EM residents. This makes it difficult to generalize the results to all of our patients. Intubations performed by experienced staff physicians could have a shorter time between apnea and first pass success, so AP OX might not be as beneficial for these patients.
Bottom Line
This study suggests that apneic oxygenation, an intervention that is relatively convenient and low-cost, may be beneficial in increasing first pass success without hypoxemia during rapid sequence intubation in the emergency department.

For an overview of core airway knowledge and skills, check out CRACKCast Episode 192 – Airway.
References
- 1.Hasegawa K, Shigemitsu K, Hagiwara Y, et al. Association Between Repeated Intubation Attempts and Adverse Events in Emergency Departments: An Analysis of a Multicenter Prospective Observational Study. Annals of Emergency Medicine. December 2012:749-754.e2. doi:10.1016/j.annemergmed.2012.04.005
- 2.Mort TC. Emergency Tracheal Intubation: Complications Associated with Repeated Laryngoscopic Attempts. Anesthesia & Analgesia. August 2004:607-613. doi:10.1213/01.ane.0000122825.04923.15
- 3.Kim WY, Kwak MK, Ko BS, et al. Factors Associated with the Occurrence of Cardiac Arrest after Emergency Tracheal Intubation in the Emergency Department. Chen X, ed. PLoS ONE. November 2014:e112779. doi:10.1371/journal.pone.0112779
- 4.Heffner AC, Swords DS, Neale MN, Jones AE. Incidence and factors associated with cardiac arrest complicating emergency airway management. Resuscitation. November 2013:1500-1504. doi:10.1016/j.resuscitation.2013.07.022
- 5.Heffner AC, Swords D, Kline JA, Jones AE. The frequency and significance of postintubation hypotension during emergency airway management. Journal of Critical Care. August 2012:417.e9-417.e13. doi:10.1016/j.jcrc.2011.08.011
- 6.Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: A justification for incorporating the ASA Guidelines in the remote location. Journal of Clinical Anesthesia. November 2004:508-516. doi:10.1016/j.jclinane.2004.01.007
- 7.Sakles JC, Chiu S, Mosier J, Walker C, Stolz U. The Importance of First Pass Success When Performing Orotracheal Intubation in the Emergency Department. Reardon RF, ed. Acad Emerg Med. January 2013:71-78. doi:10.1111/acem.12055
- 8.Sakles JC, Mosier JM, Patanwala AE, Arcaris B, Dicken JM. First Pass Success Without Hypoxemia Is Increased With the Use of Apneic Oxygenation During Rapid Sequence Intubation in the Emergency Department. Reardon RF, ed. Acad Emerg Med. May 2016:703-710. doi:10.1111/acem.12931
Reviewing With the Staff

Krista Dowhos
Latest posts by Krista Dowhos (see all)
- Teaching That Counts: Crisis Resource Management in Medical Simulation - January 8, 2021
- Teaching That Counts: Tips on Receiving Feedback - August 21, 2020
- Teaching That Counts: Diagnosing Your Learner - April 17, 2020

Latest posts by Alvin Chin (see all)
- Introducing: CRACKCast Visual Flashcards! - June 25, 2021
- PEM Pearls 03: Non Accidental Trauma pt. 2 - February 13, 2021
- PEM Pearls 02: Non-Accidental Trauma pt. 1 - January 29, 2021