
Can’t Miss Diagnoses
Central Causes
- Cerebellar hemorrhage
- Stroke (especially posterior circulation)
- Vertebrobasilar insufficiency
- Multiple sclerosis
- Trauma
- Infections
Peripheral Causes:
- Benign Paroxysmal Positional Vertigo (BPPV)
- Vestibular neuritis/ labyrinthitis
- Meniere’s Dz
- Infection: Acute otitis media
- Foreign body in the ear canal
Vertigo Mimics:
- Syncope / Pre-syncope
- Hypoglycemia
- Dehydration
Points to focus upon
Hx:
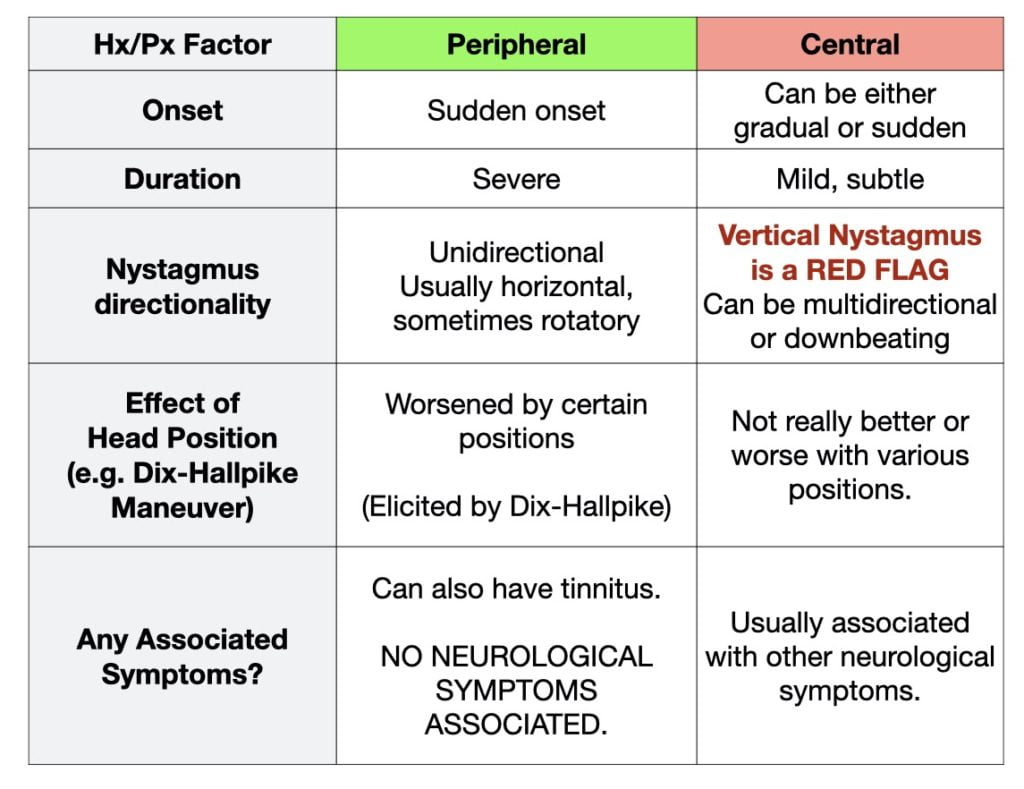
It is key to differentiate between peripheral (relatively benign, but extremely annoying) and central vertigo (possibly insidious and dangerous). See below chart for compare and contrast. History is notoriously UNRELIABLE as a differentiator for patient’s vertigo (see review article by Edlow for details).
Remember, central causes of vertigo will often have very subtle findings on a neurological screening exam (e.g. subtle gait disturbance). Be VERY CAREFUL when doing an examination on a patient. It is very easy to miss central vertigo caused by posterior circulation strokes.
Central or peripheral: Central vertigo is classically ill-defined and constant associated with vertical, bi-directional (direction changing) nystagmus. Peripheral vertigo is classically dramatic and sudden with rotatory- vertical or horizontal nystagmus and intense paroxysmal vertigo.
Px:
Beginning with ABCs, complete vitals Pulse oximeter, and fingerstick glucose.
Orthostatic vitals & cardiovascular assessment and documenting any prior history of bleeding, volume loss.
Complete neurological exam – important findings: diplopia, dysarthria, visual changes, gait, cerebellar testing (rapid alternating movements, finger-to-nose)
Including the Dix-Hallpike Maneuver and/or HINTS exam.
Clinical Decision Tools
Investigations
- CBC, BUN, Cr, Lytes, Glucose
- INR/PTT (esp if on warfarin or DOACs)
- CT Head (r/o ICH more ruling things in)
- ECG in elderly
- Consider admission or rapid follow-up for MRI of central cause suspected.
Management
Regardless of disposition, patients with dizziness should we warned NOT TO DRIVE WITH THEIR SYMPTOMS, regardless of the type of vertigo they have.
Peripheral Vertigo
The Epley Maneuver is often therapeutic – but may not always work in the ED.
Central Vertigo
Usually will usually require either admission or specialist consultation. For new CNS bleeds/lesions, neurosurgery or neurology may need to be involved for rapid intervention or close follow-up.
Recommended reading, videos, and podcasts
- Boring Question: Dizzy, need a few HINTS?
- Tiny Tip: HINTS exam to determine INFARCT
- CRACKCast E019 – Dizziness and Vertigo
- MacEmerg Podcast – Dr. Jonathan Edlow from Harvard & Dizziness (Skip to 26m15s for the Dizziness Section)
- EM Basic Podcast – Dizziness
- EM Basic Podcast Shownotes
The following is part of the CanadiEM Frontline Primer. An introduction to the primer can be found here. To return to the Primer content overview click here.
This post was copyedited and uploaded by Evan Formosa.

Afsheen Mehar
Latest posts by Afsheen Mehar (see all)
- CanadiEM Frontline Primer – Incision and Drainage - April 26, 2020
- CanadiEM Frontline Primer – Suturing and Wound Closure - April 26, 2020
- CanadiEM Frontline Primer – Early Pregnancy – First Trimester Bleeding - April 25, 2020

Teresa Chan
Latest posts by Teresa Chan (see all)
- 2021 CanadiEM Year in Review and Editor’s Choice Awards - January 4, 2022
- 2020 CanadiEM Year in Review and Editor’s Choice Awards - January 1, 2021
- Virtual Retreat 2020: The Future of CanadiEM - October 22, 2020