
Can’t Miss Diagnoses
- Sepsis (obviously) – but critically important to find the source and control it!
- Meningitis / Encephalitis (Not to miss since may need LP for full diagnosis)
- Febrile neutropenia (especially if recent chemotherapy)
- Alcohol Withdrawal (hyperthermia, tachycardia, diaphoresis)
- Benzodiazepine Withdrawal (hyperthermia, tachycardia, diaphoresis)
- Toxic ingestions – cocaine, methamphetamines, crystal meth
- Thyroid Storm
- Serotonin Syndrome
- Neuroleptic malignant syndrome
Points to focus upon
Approximately 0.5% of ED visits are related to sepsis, with the majority of cases (55-70%) occurring in patients 60 and older.1,2 Most patients diagnosed with sepsis are admitted to hospital (75-90%), with up to a third of these patients admitted to ICU. Septic shock is a rare (<5%) but serious complication.2
Resuscitation Needs
IV, O2, monitoring and complete vitals.
Hx:
Recognizing the source of infection, travel, immunocompromised status and sick contact history.
Remember: Not all fever is from an infectious source. Some non-infectious causes of fever: PE, thyrotoxicosis, crystal arthropathy, toxic ingestions, withdrawal syndromes, etc.
Also Remember: Not all septic patients have a fever. Those without fever have been shown to have worse in-hospital outcomes.
Approach
Often vague initial presentation with broad differential in older patients, however, it is critical to initiate empiric therapy as soon as possible. Therefore having a high index of suspicion is important, particularly in vulnerable populations (e.g. advanced age, immunosuppressed, diabetes, malignancy, recent hospitalization).
Considerations in the age of COVID-19 for your safety:
Not all COVID-19 patients will present with fever and cough, and older patients can often present atypically. If the rate of COVID-19 is high in your community, take appropriate precautions when assessing patients with concern for sepsis or other infectious syndromes.
Investigations
- CBC, BUN, Cr, Lytes, Glucose, VBG
- Consider NPS, Blood Cultures
- Consider CXR, Urinalysis (+/- culture),
- Imaging based on suspected source of infection – e.g. CNS imaging (brain, spine), CT KUB for Septic urolithiasis, Ultrasound of biliary tree for cholangitis/cholecystitis, CT Abdo/Pelvis for other intraabdominal sources.
Consider adding the following:
- Troponin / ECG – depending on suspicion for end-organ dysfunction
- Liver enzymes – – depending on suspicion for end-organ dysfunction
- Liver function tests (Bilirubin, INR, Albumin, Glucose) – depending on suspicion for end-organ dysfunction
- Lipase
If coagulopathy suspected, may want to consider:
- INR/PR
- PTT
- Fibrinogen
- D-Dimer
Clinical Decision Tools
Sepsis Scores
- qSOFA Mnemonic -HAT (Hypotension, AMS, Tachycardia)
- SOFA (current criteria – surviving sepsis 2016)
- NEWS
- NEWS2 (Most recent criteria – calculated at triage without bloodwork)
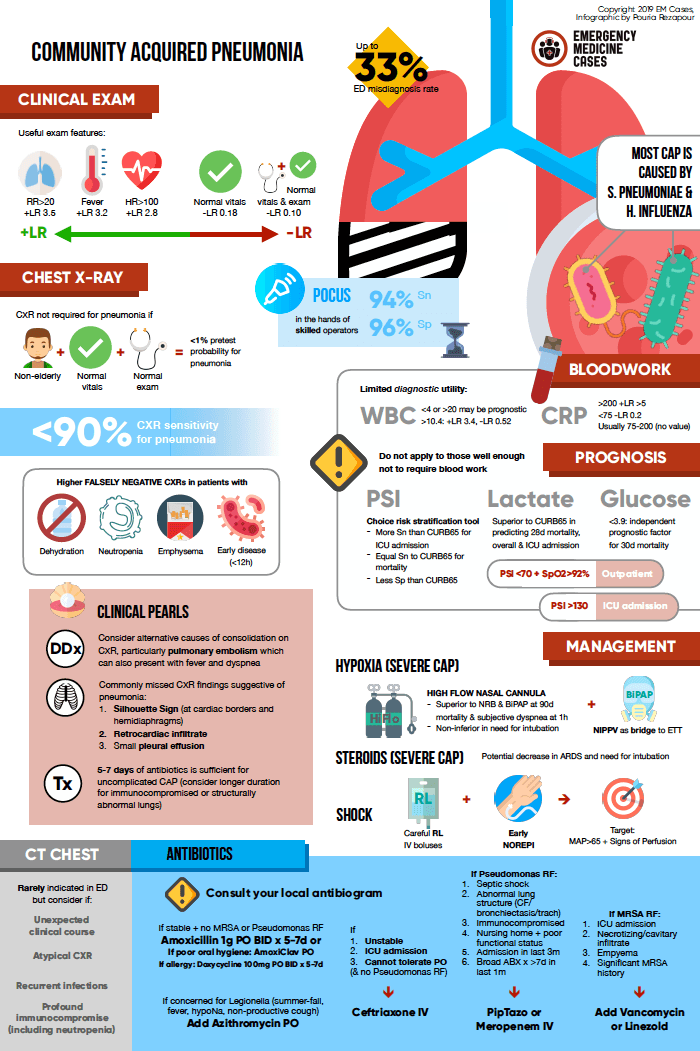
Pneumonia Scores
- PSI (Pneumonia Severity Index) Score
- CURB-65 Score
- MuLBSTA – Mortality for Specifically Viral Pneumonia – launched during COVID-19 – yet to be externally validated.
Management
The mainstay of sepsis resuscitation is:
1) Supportive measures (including fluid resuscitation and intubation as needed);
2) Early antibiotics and/or source control.
Fluid resuscitation should be targeted to support perfusion of end-organs. And vasoactive agents (a.k.a. “pressors”) can be used to help as well, and maybe started peripherally (yes, even norepinephrine).
The first choice fluid is currently Ringer’s Lactate for large-volume fluid resuscitation. Please see below for First 10:EM summaries of the three recent IV Fluids Papers (SPLIT, SMART, and SALT-ED).
For patients with COVID-19 (or suspected COVID-19), conservative fluid resuscitation and early use of vasoactive agents is advised since higher volumes of fluids may be harmful. See the JAMA SSC Summary (Published March 26, 2020).
Recommended reading, videos, and podcasts
- CRACKCast E012 – Fever in the ER
- CRACKCast E138 – Sepsis Syndromes
- CanadiEM COVID-19 Summary of SSC Recommendations
- Quick ICU training – Sepsis Infographics
- First 10:EM IV Fluids Week Posts:
- EM Cases – Community-Acquired Pneumonia: Emergency Management
- EM Cases – Community-Acquired Pneumonia infographic
- CRACKCast E023 – Sore Throat
- CRACKCast E109 – CNS Infections
- CRACKCast E075 – Upper Respiratory Tract Infections
{kind=link}
The following is part of the CanadiEM Frontline Primer. An introduction to the primer can be found here. To return to the Primer content overview click here.
This post was edited by Dr. Sonja Wakeling MD. This post was copyedited and uploaded by Evan Formosa.
References
- 1.Strehlow MC, Emond SD, Shapiro NI, Pelletier AJ, Camargo CA Jr. National Study of Emergency Department Visits for Sepsis, 1992 to 2001. Annals of Emergency Medicine. September 2006:326-331.e3. doi:10.1016/j.annemergmed.2006.05.003
- 2.Wang HE, Jones AR, Donnelly JP. Revised National Estimates of Emergency Department Visits for Sepsis in the United States*. Critical Care Medicine. September 2017:1443-1449. doi:10.1097/ccm.0000000000002538

Afsheen Mehar
Latest posts by Afsheen Mehar (see all)
- CanadiEM Frontline Primer – Incision and Drainage - April 26, 2020
- CanadiEM Frontline Primer – Suturing and Wound Closure - April 26, 2020
- CanadiEM Frontline Primer – Early Pregnancy – First Trimester Bleeding - April 25, 2020

Ryan O'Reilly
Latest posts by Ryan O'Reilly (see all)
- CanadiEM Frontline Primer – Lower Leg Swelling - April 25, 2020
- CanadiEM Frontline Primer – Fever & Sepsis - April 25, 2020
- CanadiEM Frontline Primer – Pulmonary Embolism - April 25, 2020

Teresa Chan
Latest posts by Teresa Chan (see all)
- 2021 CanadiEM Year in Review and Editor’s Choice Awards - January 4, 2022
- 2020 CanadiEM Year in Review and Editor’s Choice Awards - January 1, 2021
- Virtual Retreat 2020: The Future of CanadiEM - October 22, 2020