

This episode of CRACKCast covers Rosen’s Chapter 23, Sore Throat. While the sore throat may have some relatively benign causes, knowing the red flags for this common complaint will have you saying “ahhh” as you diagnose the more serious pathology in the ED.
Shownotes – PDF Here
[bg_faq_start]Rosen’s in Perspective
Relevant Anatomy
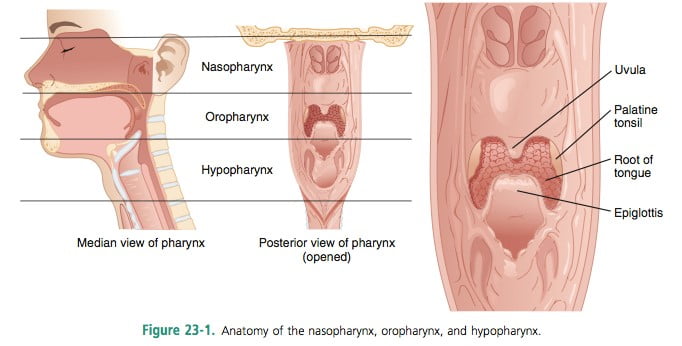
One of the most common chief complaints in the ED, sore throat or pharyngitis is caused by inflammation of the pharynx (at any level).
[bg_faq_end][bg_faq_start]1) List 8 Emergent Diagnosis for Sore Throat
Diseases not to miss:
- Epiglottitis
- Bacterial tracheitis
- Ludwig’s angina
- Gonorrhoea
- Foreign body
- Angioedema
- Peri-tonsillar abscess
- Retro-pharyngeal abscess
- Primary HIV
- Corynebacterium Diphtheriae
- Epstein barr virus
- Cancer
- Herpes Simplex
2) List the most common viral, bacterial, and non-infectious causes of sore throat (list at least 8)
Viral – The most common cause of acute pharyngitis
- Rhinovirus
- Adenovirus
- HSV 1&2
- EBV
- Influenza
- CMV
- Varicella-zoster virus
- Hepatitis virus
Bacterial
- Group A Beta-Hemolytic streptococcus
- Non-group A streptococcus
- Neisseria gonorrhoeae
- Neisseria meningitidis
- Mycoplasma pneumoniae
- Chlamydia trachomatis
- Corynebacterium diphtheriae
- influenzae
Non-infectious causes:
| Systemic Diseases | Trauma | Tumours |
| o Kawasaki’s disease o SJS o Cyclic neutropenia o Thyroiditis
| o Retained foreign body o Laryngeal fracture o Hematoma o Caustic exposure o Post-tonsillectomy eschar | o Tongue o Larynx o Thyroid o etc.
|
3) Describe the Centor Criteria and their use
Lets take a step back and talk about the airway red flags when it comes to sore throats:
- Rapidly progressive symptoms
- Unwell, restless, distressed
- Hypoxia
- Drooling
- Muffled voice (supraglottic threat)
- Stridor (means glottic problem – common in children <10 with croup)
- Dehydration and systemic toxicity
- “Brawny” induration on the floor of the mouth
- Direct visualization paramount
- Trismus vs. bilateral tonsillar exudates vs. uvular deviation vs. signs of PTA
See: http://www.mdcalc.com/modified-centor-score-for-strep-pharyngitis/
Viral vs. Bacterial Differentiation
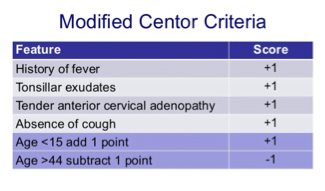
Modified CENTOR criteria scoring
If ≥4 points on the scale…
… only 51% Group A strep infection (not good)
- All USED to get antibiotics
From MDcalc Description:
“The Modified Centor Criteria (or McIsaac Score) correlate directly with risk of positive throat culture for GAS.”
- The “Modified” criteria include an age component, along with “tonsillar swelling” as part of the rule. GAS is incredibly rare in patients under 3 and less common in older adults, so this can help risk stratify patients for clinicians.
- Most cases of pharyngitis are viral in origin, and with the rare incidence of rheumatic fever, along with the questionable benefits of early antibiotics to prevent sequelae like peritonsillar abscess, antibiotics are prescribed much less often. Steroids (like dexamethasone) and NSAIDS often provide similar pain relief and resolution of symptoms to antibiotics.”
Wisecracks
[bg_faq_start]1) Describe the pros and cons of antibiotics for suspected or confirmed acute GAS pharyngitis
- See rosen’s page 202
Antibiotics: Only reduce GAS symptoms by 16 hours.
From Rosen’s Page 202
- Only gonococcal disease should be treated with antibiotics
- Antibiotics only useful in reducing rheumatic fever during one military epidemic in the 20th century, and the decline of rheumatic fever is due to industrialization, hygiene, living conditions, access to care, and nutrition. Therefore they ought only to be used in endemic or epidemic settings.
- Antibiotics do NOT reduce the incidence of suppurative complications from sore throat (e.g. peritonsillar abscess)
- Key to management is thorough patient education and explanation of:
- The natural disease course of infectious pharyngitis
- Encourage symptomatic treatment (NSAIDS and steroids)
- Antibiotic risks: anaphylaxis, resistance, n/v/d, rash
Some debate the safety of the no “antibiotic approach” but:
“However, the signs and symptoms of streptococcal and non-streptococcal pharyngitis overlap too broadly for diagnosis to be made with the requisite diagnostic precision on the basis of clinical grounds alone. Even subjects with all clinical features in a particular scoring system can be confirmed to have streptococcal pharyngitis only about 35%–50% of the time, and this is particularly the case in children. The clinical diagnosis of GAS pharyngitis cannot be made with certainty even by the most experienced physicians, and bacteriologic confirmation is required.” – IDSA Guidelines 2012
Read more about this here:
[bg_faq_end][bg_faq_start]2) Other than Group B strep, name 6 agents causing exudative tonsillopharyngitis
- Group A Streptococcus
1b) Non-group A strep - Neisseria gonorrhoea
- EBV / Mono
- Haemophilus influenzae
- Cornybacterium diphtheriae
- Candida species (?HIV infection)
- Mycoplasma pneumoniae
- Chlamydia trachomatis
- Pneumoniae
- Necrotizing tumour
- Post tonsillectomy eschar

Adam Thomas
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018