
This year, CanadiEM has partnered with the Canadian Association of Emergency Physicians, EMOttawa, and the Skeptic’s Guide to Emergency Medicine to help promote #CAEP21: CAEP at the Forks – Rising to the Challenge. From June 15-17, 2021 we will be publishing The CAEP Daily, a journalistic summary of highlights from the conference. Please join the discussion!
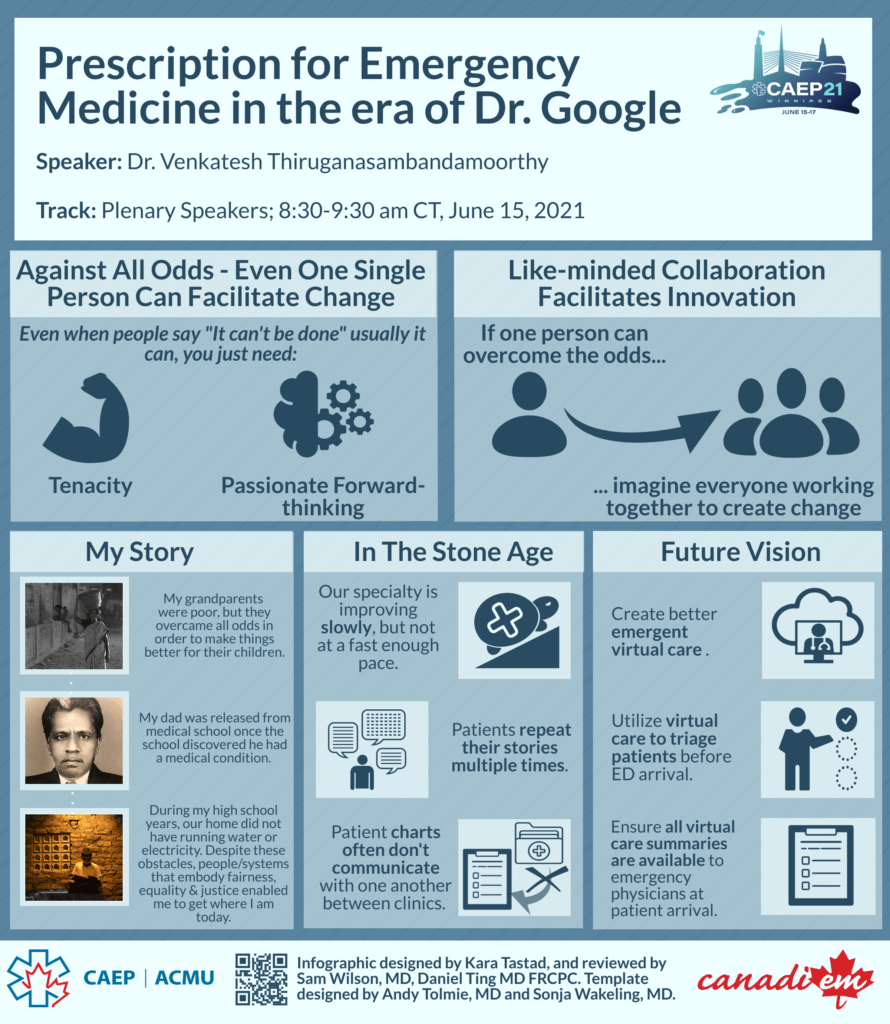
[bg_faq_start]Today’s Plenary Speakers:


Here’s what else you need to know today:
Ethics – Panel Discussion: High-Risk Addictions, Capacity Assessment, and Forced Treatment
Moderated by Dr. Merril Pauls; Speakers: Dr. Aaron Orkin & Dr. Anas Manouzi
There’s a push, especially in paediatrics, for involuntary admission to help stabilize patients and start them on opioid agonist therapy. But there’s harm to be considered with blanket involuntary admissions for all. Patients who are forced into treatment can develop negative associations with the healthcare system. Furthermore, we need to consider the transition to and development of outpatient services after an admission.
We need to frame overdoses just like we do any medical or mental health emergency. We know that key interventions like opioid agonist therapy and naloxone kits can save lives. Care providers should be initiating buprenorphine/naloxone, providing opioid agonists in the department, and sending patients home with naloxone kits. Emergency medicine is a population-based specialty and providing access to screening, treatment, admission when necessary is part of our duty of care.
Ethics – Lessons Learned from COVID
Track Co-Chairs: Dr. David Migeault, Dr. Merril Pauls; Panelists: Dr. Jolion McGreevy, Dr. Marie-Maud Couture, Dr. Francis Bakewell, Dr. Jacqueline Willinsky.
Healthcare providers globally have experienced significant moral distress during the COVID-19 pandemic. In the early stages, there was limited information and a lack of evidence about what type of personal protective equipment (PPE) would be effective against the virus, leading to worry about whether resources would last and what would happen if they ran out. Being prepared to make decisions in high acuity COVID situations became a regular occurrence, and these decisions became increasingly centred on ethics.
But the pandemic has also demonstrated incredible teamwork amongst specialties and allied health. Palliative care physicians have assisted with more robust goals of care discussions, ensuring care is prioritized based on patient values. Having multidisciplinary teams in the ED to help make real-time decisions was invaluable during case surges. For staff, wellness initiatives included a “buddy system,” where providers were paired and could debrief about challenging encounters. Peer support systems using this buddy model were deemed to be more effective than formal mental health initiatives at these institutions.
We should be proud of our accomplishments. Being on the frontlines fighting a battle with such limited information, being pioneers in the first phase of the crisis, and being the definition of what it means to collaborate and rise to the occasion. Emergency departments across the globe are enhanced for the leadership and sacrifice made by all healthcare providers.
Climate Change – Planetary Health, & A Healthy Recovery From COVID-19
Speaker: Dr. Courtney Howard
Our healthcare system is built on the social and structural determinants of health, which in turn rests on ecological determinants of health. As emergency physicians, we must learn our role in advocating for change to improve health outcomes for patients in the future.
Immediate and direct risks of climate change on patient health include asthma in wildfire smoke inhalation, injuries from severe storms, and communicable disease borne by migrating insect vectors. These, along with indirect risks to health like poor crop yields, population displacement, and conflict wars are only worsening as our planet warms.
Canada is warming at twice the rate of global warming. Dr. Howard argues that we have an obligation to advocate for divestment in fossil fuels, act as role models for patients, learn more about Bill C-12 (national targets for greenhouse gas emissions), and join the charge towards net zero emission healthcare.
Rural Medicine – Use of Turkel Safety Needles in the ED
Speaker: Dr. Sean Moore
Turkel needles can be used for many indications, including to perform a needle thoracostomy, thoracentesis, and paracentesis. These needles have 5 main advantages over others:
- Combination of blunt and sharp needle when entering into a cavity.
- There are easy to see when through a chest or abdominal wall.
- They can be visualized on ultrasound.
- They have a one-way value which is valuable when used to relieve a tension pneumothorax.
- They are actually long enough to use for a needle thoracostomy in the traditional decompression location.
Rural Medicine – Metallic Foreign Bodies in the Eye
Speaker: Dr. Sarah Giles
Take Home Points:
1. Treat acute pain with topical anesthetic, and be mindful not to give patients large quantities of anesthetic to take home for relief (the remaining few drops in the single-use dropper will suffice).
2. Topical NSAIDs do not work better than oral options.
3. After care: Only 14% of foreign bodies are culture positive, so antibiotics are not always needed. Corneal wounds recover better when moist. You must cover pseudomonas if the patient is a contact lens wearer, and they require good return to Emergency Department instructions if their condition worsens.
Pediatric Pearls – More Than Just Gastro: Vomiting in Infants
Speaker: Dr. Sarah Reid
In the first few weeks of life, billious vomiting may appear yellow rather than green, and anything other than milk colour is potentially concerning. Another key aspect in the history is the pattern of vomiting. A benign issue like reflux is usually intermittent; there should be normal feeds in between episodes of vomiting. When vomiting is with every feed or showing a progressive pattern, you should think about more dangerous diagnoses such as pyloric stenosis, malrotation or intussusception. One key pearl is to observe the infant feeding in the emergency department, which also gives you a period of observation. For patients who are discharged, it is very important to invest the time necessary to ensure parents understand instructions around reasons to return, including if the pattern of vomiting worsens.
Core EM – Vertigo
Speaker: Dr. Peter Johns
The HINTS exam should only be done on patients with acute vestibular syndrome (constant dizziness). The most challenging part of the exam is the head impulse test. Keep a firm grasp on the patient’s skull (not the mandible) and start with slow movements to loosen the patient’s neck up. Then turn the patient’s head 20 degrees off midline and rapidly bring it back with a sharp endpoint. A catchup saccade would suggest a peripheral cause.
Vestibular migraines are the second most common cause of vertigo but the diagnosis is rarely made in the ED. Patients can be dizzy for as little as a few minutes but as long as three days. While they may not have a headache, they will often have other migrainous features such as photophobia, phonophobia, visual aura, and history of multiple similar episodes. Treatment for vestibular migraine is similar to that of a normal migraine and often includes metoclopramide.
Check out this talk, the CAEP procedure talk on how to do a Dix-Hallpike, this article for worrisome central features, and Dr. Johns’s YouTube channel for essential vertigo pearls.
Core EM – Endocarditis
Speaker: Dr. David Carr
Diagnosing endocarditis can be challenging. “Unusual” patient groups that are at risk of endocarditis include patients with cancer and with lupus. Classic signs like Osler nodes, Janeway lesions, and Roth spots are rare. Instead, we should value dental findings and/or history of dental procedures or cleanings within the last 2 weeks. The mouth is fortunately easy to examine.
In healthy patients, coagulase-negative Staphylococci growing in blood cultures are usually contaminants. However, in patients with heart valve replacements, the diagnosis of endocarditis needs to be considered. In patients with valve replacements, coagulase-negative Staphylococci are the second most common culprit of endocarditis.
Further reading:
- CAEP Conference website
- EM Ottawa on the CAEP Conference
- Skeptic’s Guide to Emergency Medicine
- Learn more about CanadiEM’s Virtual Community of Practice
- Call for CanadiEM Junior Editors, deadline June 30, 2021!
This post was copy edited and uploaded by Kara Tastad

Hans Rosenberg
Latest posts by Hans Rosenberg (see all)
- The CAEP Daily: Day 3 (June 17) - June 17, 2021
- The CAEP Daily: Day 1 (June 15) - June 15, 2021
- CAEP 2021: Recent EM Literature and Global EM Tracks - June 10, 2021

Sonja Wakeling
Latest posts by Sonja Wakeling (see all)
- The CAEP Daily: Day 2 (June 16) - June 16, 2021
- The CAEP Daily: Day 1 (June 15) - June 15, 2021
- 2020 American Heart Association Guidelines for Education Science - December 2, 2020

Alkarim Velji
Latest posts by Alkarim Velji (see all)
- The CAEP Daily: Day 3 (June 17) - June 17, 2021
- The CAEP Daily: Day 2 (June 16) - June 16, 2021
- The CAEP Daily: Day 1 (June 15) - June 15, 2021

Patrick Boreskie
Latest posts by Patrick Boreskie (see all)
- The CAEP Daily: Day 3 (June 17) - June 17, 2021
- The CAEP Daily: Day 2 (June 16) - June 16, 2021
- The CAEP Daily: Day 1 (June 15) - June 15, 2021

Daniel Ting
Latest posts by Daniel Ting (see all)
- Dress for Success: A Guide to Dressing Choices for Common Wounds in the Emergency Department - April 25, 2024
- 2023 CanadiEM Year in Review and Editor’s Choice Awards - January 2, 2024
- Call for Junior Editors, Class of 2023-24 - September 21, 2023