

In Part One of this series, we reviewed the pathophysiology of Acute Coronary Syndromes (ACS), as well as some of the important features that should be elucidated on history-taking. In Part Two we discussed the current evidence-based practices for the management and transportation considerations in patients identified by paramedics to be suffering from a STEMI. In this third part, we will consider the series of events that occur when the care of a patient with suspected ACS is transferred to the ED.
[bg_faq_start]About Sirens to Scrubs
Sirens to Scrubs was created with the goal of helping to bridge the disconnect between pre-hospital and in-hospital care of emergency patients. The series offers in-hospital providers a glimpse into the challenges and scope of practice of out-of-hospital care while providing pre-hospital providers with an opportunity to learn about the diagnostic pathways and ED management of common (or not-so-common) clinical presentations. By opening this dialogue, we hope that these new perspectives will be translated into practice to create a smoother, more efficient, and overall positive transition for patients as they pass through the ED doors.
[bg_faq_end]Objectives:
- To understand how ACS is diagnosed
- To learn about emergency department management of ACS and post-ACS therapies
As we discussed last month, standard-of-care for many ambulance services is to bring patients suffering from a STEMI directly to the catheterization lab for primary PCI (percutaneous intervention) or to treat them with thrombolysis in the field. Fortunately, only a handful of patients complaining of chest pain have a clear STEMI on their pre-hospital ECG; so how are the rest worked-up and managed in the Emergency Department?
Diagnosis of ACS
Myocardial infarction (STEMI or nSTEMI)
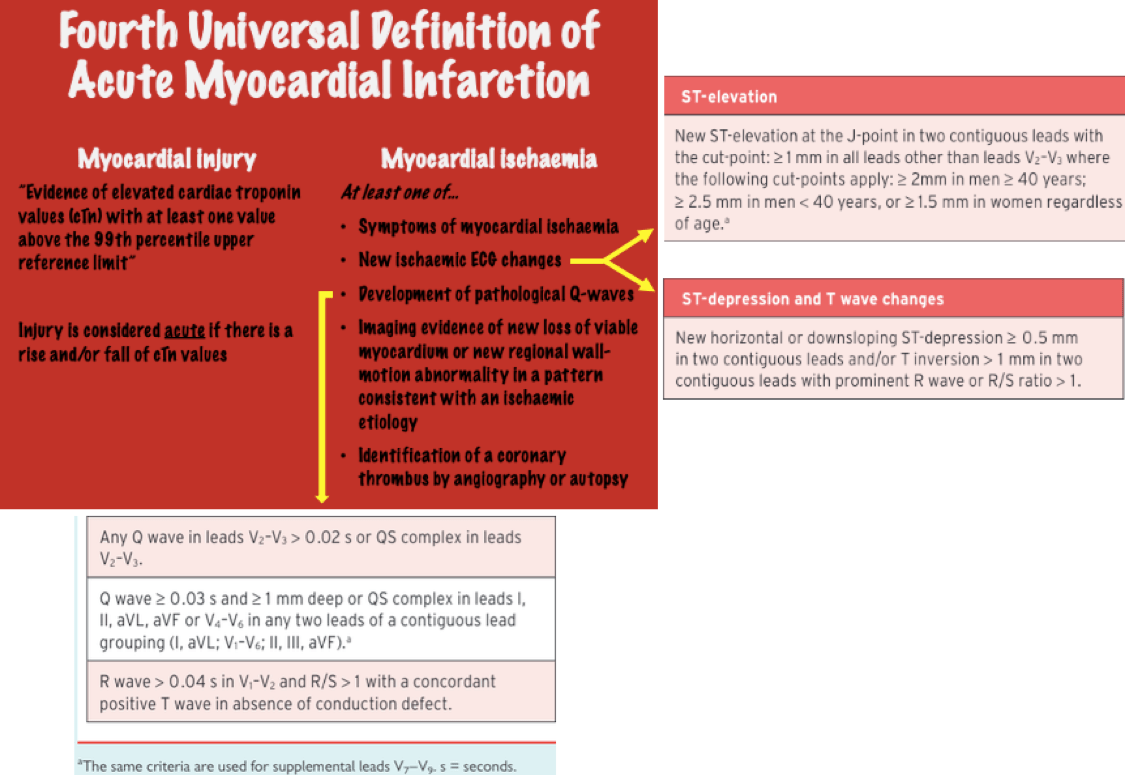
In 2018 the Fourth Universal Definition of Myocardial Infarction was published, which defined an acute myocardial infarction as “Acute myocardial injury with clinical evidence of myocardial ischaemia”.1 Myocardial injury and myocardial ischemia are further defined…
Unstable angina
As we explained in Part One, Unstable Angina describes symptoms of myocardial ischemia +/- ECG changes in the absence of elevated serum troponin levels. Unstable angina is further defined to differentiate it from stable angina, a non-acute coronary syndrome condition which can have symptoms similar in nature to ACS. Angina is considered “unstable” if:2
- It occurs with rest or minimal exertion and lasts longer than 20min
- It is new-onset and severe (Canadian Cardiovascular Society grade III or IV – onset with walking 1-2 level blocks or 1 flight of stairs)
- Crescendo angina – previously diagnosed angina that has become more frequent, more severe in quality, or precipitated by less severe levels of exertion.
Types of MI
While paramedics are most familiar with ACS that has been caused by acute rupture of a plaque with subsequent thrombus development, this is actually only one mechanism of MI (Type 1). The other clinically significant mechanism of MI (Type 2) is caused by a supply-demand mismatch, which can occur from sustained tachyarrhythmias, severe anemia, profound hypotension, just to name a few specific mechanisms. Click here to read more about the types of MI, including criteria for a Silent MI (page 5 of the document). Below are some nice images from the Fourth Universal Definition of Myocardial Infarction that demonstrate ways in which a Type 1 or 2 MI can occur:1


Cardiac biomarkers
Cardiac biomarkers are proteins that are identified on bloodwork that are suggestive of myocardial injury. Biomarkers have been used in the diagnosis of MI since the 1960s, however, the first biomarkers (aspartate transaminase [AST], lactate dehydrogenase [LDH], and creatine kinase [CK]) were very non-specific to the heart (many other tissues released them).3 Over time, more specific biomarkers were found (CK-muscle/brain [CK-MB], LDH 1 + 2, and myoglobin), however, high false-positive results continued to be an issue until an assay was developed to identify cardiac-specific troponins in the blood. If you recall, troponins are proteins that play a key role in muscle contraction, both in skeletal and cardiac muscles. There are three types of troponin, C, I, and T – both I and T have isoforms that are very specific to cardiac muscle, and thus, the presence of these isoforms (called cardiac troponins) is suggestive of myocardial injury when the patient’s symptoms and/or ECG support this diagnosis.
When a patient presents with suspicion of an acute coronary syndrome, their blood is sent to the lab to look for elevated levels of these troponins. Unfortunately, the troponin level doesn’t rise as soon as the myocardium is injured; rather, it takes 4-8h to start seeing it elevated in the blood. It’s for this reason that a single troponin result that is within normal limits cannot usually be used to exclude myocardial injury. Current North American guidelines recommend that troponin levels be tested at least twice before ruling out myocardial infarction – once as soon as feasible after the patient arrives at the emergency department, and subsequently 3 to 6hrs later.4
It is important for paramedics to explain to patients what to anticipate when they go to the ED with chest pain or other symptoms suspicious for ACS. By setting reasonable expectations with regards to how long the ED visit might take patients can plan appropriately and are apt to be less frustrated when it happens. The graph below demonstrates the approximate timelines of troponin elevations in different sized MIs – note that, while the troponin level rises rapidly above the 99th percentile, it isn’t immediate at the time of infarct.5 Note also that troponin remains elevated in the blood for 7-10 days after onset of infarct, which allows later presentations of MI to potentially be diagnosed in the ED.

MONA3
Whether a patient diagnosed with ACS is treated with primary PCI, thrombolysis, or neither, they receive (approximately) the same emergency therapies upon diagnosis at the hospital. First off, all the same discussion we had around MONA in Part One of this series holds true for ED management of ACS as well. Three additional therapies are often added to this regimen in the ED:
- Anti-platelet agent – a second P2Y12 inhibiting agent is usually added. Depending on your centre, this may be clopidogrel (Plavix), ticagrelor (Brilinta), or prasugrel (Effient).
- Anti-coagulant – to directly target the coagulation cascade. Depending on your centre, type of ACS, and patient factors, providers may opt for unfractionated heparin, low molecular weight heparin (Enoxaparin, Dalteparin), or Fondaparinux
- Antagonist of GP IIb/IIIa (Abciximab) – if you remember back, this is the receptor that acts as the final pathway in the activation of platelets. In blocking this receptor, platelet aggregation can be further reduced. These agents are indicated only in very specific presentations of ACS.6
Post-ACS Care
So, you successfully assessed and treated your ACS patient in the field and transported them to the appropriate facility. From there, appropriate emergency therapies were initiated and your patient was admitted to the hospital for stabilization and to organize post-ACS care. But what does that involve? First off, there is a list of medications that almost all patients who suffer and ACS event will be discharged on – these include:78
- ASA – forever. Enough said.
- P2Y12 inhibitor (clopidogrel, ticagrelor, prasugrel) – typically for at least a year unless they have significant bleeding complications.
- Beta blockers (metoprolol, carvedilol, bisoprolol) – reduce long-term mortality after MI by 23%. Many patients will require these for life unless adverse effects (low energy, falls) or contraindications (bradycardia, hypotension, high-grade AV block) develop. Mechanisms for mortality-reduction may include:
- By decreasing inotropy (force of contraction) and chronotropy (heart rate), myocardial demand is lowered
- Decreased risk of lethal arrhythmias
- Remember that the heart is perfused during diastole; a heart that is pumping at a slower rate spends more time in diastole and thus the heart spends more time being perfused
- Reduced adverse remodeling. This one requires some physics to truly understand, but essentially, in the period immediately after an MI, a damaged heart changes its structure to adapt to the loss of healthy myocardial tissue. However, when this remodeling process continues over the long-term, changes to the heart shape, size, and wall thickness lead to myocardial dysfunction and congestive heart failure. Beta blockers are one class of medication demonstrated to interfere with the remodeling process.
- Statins (atorvastatin, rosuvastatin, pravastatin) – by blocking the HMG CoA reductase enzyme, statins decrease cholesterol formation in the liver. In addition, statins have been shown to moderate inflammation, oxidative stress, thrombus formation, and endothelial dysfunction.9 These are also for life unless adverse effects develop (most commonly, muscle pain).
- Angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) – lower blood pressure and also interfere with the remodeling process described above. Also for life unless adverse effects (of which serious side effects may include angioedema or hyperkalemia and a common side effect is a persistent cough).
In addition to their new pharmacy, patients being discharged after an ACS event should also receive information about the following:
- Lifestyle modifications (i.e. quit smoking, engage in at least 150min/week of moderate-intensity aerobic exercise, promote a healthy diet, such as a Mediterranean diet)
- Exercise-based cardiac rehabilitation
- Follow-up appointments with a community cardiologist to manage their new cardiac medications and arrange for any follow-up testing that may be required.
That’s it for now! Tune in for the final installment of this series to learn about angiography and play “spot the lesion”! In the meantime, find more Sirens to Scrubs articles here!
As always, if you have any questions, thoughts, alternative perspectives, or requests for future topics, feel free to comments below or send me an email at [email protected]. Please keep in mind that, although I will do my best to publish information that is accurate across Canada, there will inevitably be some regional differences in both pre-hospital and in-hospital management of emergency patients. As a paramedic and Emergency Medicine resident in Ontario, some posts may wind-up being somewhat Ontario-centric, hence, I encourage anyone whose experiences differ from mine to contribute to the conversation by commenting below.
References
Paula Sneath
Latest posts by Paula Sneath (see all)
- Sirens to Scrubs: COVID-19, an excuse to talk about infection control - April 20, 2020
- Sirens to Scrubs: Fever-Phobia - August 20, 2019
- CAEP FEI | GridlockED: An Emergency Medicine Game and Teaching Tool - June 28, 2019