
All the content from the Blood & Clots series can be found here.
CanMEDS Roles addressed: Medical expert, scholar
Main Messages
- Improved technology has led to an increase in the detection of subsegmental PE (SSPE)
- An algorithmic approach can help identify patients who will benefit from anticoagulation: generally those with concomitant DVTs and patients with additional risk factors for progression
- There is clinical equipoise regarding the decision to anticoagulate in this case, and more research is eagerly awaited.
Case Description
A 65-year-old male presents to the emergency department complaining of chest pain three days after discharge for an open cholecystectomy for recurrent choledocholithiasis. His past medical history is significant for hypertension managed with ramipril 5mg po daily. He describes 24 hours of shortness of breath on exertion.
On exam, his BP is 140/80, HR 95, oxygen saturation 96% on room air and weight 70kg.
His cardiac and respiratory exams are within normal limits. His abdominal exam shows healing suture sites and mild tenderness to palpation diffusely without rebound or guarding.
A CT scan is performed and shows a subsegmental pulmonary embolus (SSPE) in the right lower lobe.
Main Text
This case raises the following questions:
· Which patients with SSPE will benefit from therapeutic anticoagulation?
· In patients with SSPE, what risk factors predict recurrence?
What is Subsegmental Pulmonary Embolus?
SSPE is a pulmonary embolism located in the subsegmental branches of the pulmonary arteries.
There is controversy about whether anticoagulation therapy is needed for SSPE.
Why? First, these very small filling defects may in fact be radiographic artifacts rather than true thrombi, and their clinical significance is uncertain. The improved diagnostic capabilities of modern CT scanners have led to better resolution of these small filling defects which were not detected in older diagnostic studies for PE.1,2
Second, a true subsegmental PE may be due to a small DVT, and the risk of recurrent VTE without anticoagulation may be lower than in patients with a more proximal PE.3
For these reasons, the natural history (likelihood of recurrent VTE) of untreated isolated SSPE is unclear. There is an ongoing prospective cohort study evaluating the safety of withholding anticoagulation in patients with SSPE and negative bilateral doppler ultrasounds.4
How to approach the management of SSPE: A simplified approach can be found in the figure below. When faced with a patient who presents with SSPE, clinicians have two challenges: establishing an accurate diagnosis of PE and selecting the appropriate patients who require anticoagulation.
We recommend that patients with SSPE receive anticoagulation in the following circumstances:
· Patients with concomitant deep vein thrombosis:
Rates of concomitant proximal lower limb DVT have been reported in 7.1% of patients diagnosed with SSPE. 4 Lower-extremity ultrasonography to rule out DVT should be performed in patients with SSPE. If a DVT is found, the patient will require therapeutic anticoagulation.
· Patients at high risk of recurrence:
Patients with active cancer who have SSPE should receive standard anticoagulation therapy. A recent cohort study in cancer patients who received anticoagulation for incidentally detected PE suggested that the risk of VTE recurrence was similar for subsegmental and non-subsegmental PE, which likely reflects their ongoing thrombotic risk.
Numerous other risk factors for recurrent VTE in SSPE have been proposed by the American College of Chest Physicians (ACCP) to help clinicians stratify risk. These include current hospitalization, immobility 5, and previous unprovoked VTE.3 The ACCP guidelines favour anticoagulation in these situations.
If we are waiting for an outpatient leg ultrasound (US), should these patients receive anticoagulation therapy?
If there are concomitant signs and symptoms of DVT but US access is delayed, anticoagulation therapy is recommended.
However, if there are no signs of DVT then the decision about whether to provide anticoagulation should be made on a case-by-case basis taking into account the high-risk features mentioned above, along with local access to US, access to expedited outpatient follow-up, patient comorbidity (ex. respiratory capacity), and patient preference.
At our centre, low-risk patients with isolated SSPE typically would not receive empiric anticoagulation. However, we have rapid access (within 12-24 hours) to leg ultrasound along with expedited VTE/GIM clinic follow up.
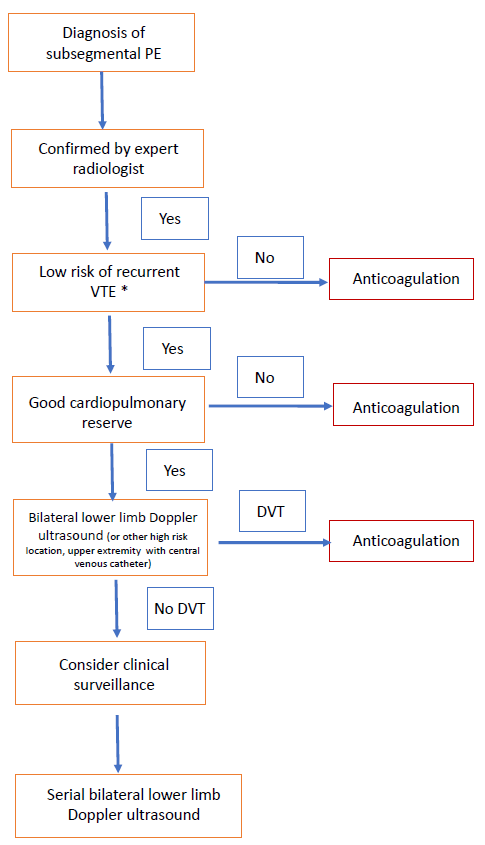
*Patients at low risk of recurrence are those who do not have recent hospitalization, immobility, active cancer (especially metastatic disease or ongoing chemotherapy).
If I decide to anticoagulate, what agent do I use for initial therapy?
The most recent ACCP guidelines recommend the use of direct oral anticoagulants to treat acute VTE, as long as there is no contraindication to these agents.3 See our previous post for more information.
What should I do if the patient’s leg dopplers are negative for DVT and we decide NOT to anticoagulate our patient (expectant management)?
Patients who do not meet criteria for treatment should be closely monitored and advised on the symptoms of DVT and PE.
If the decision is made not to anticoagulate, clinicians should consider repeating Doppler US examination of the legs within 5-7 days to detect (and treat) evolving proximal DVT. Such patients should have close follow-up with an internal medicine specialist, thrombosis clinic, or hematologist and be counseled on the signs and symptoms of DVT and PE.
Case Conclusion
This patient has symptomatic post-operative subsegmental PE. Bilateral Doppler ultrasound of the lower extremities showed no evidence of proximal DVT. No anticoagulation was started as he had no risk factors for recurrence including cancer, prior VTE, or prolonged immobilization.
The patient was seen again in follow-up 7 days later and bilateral leg ultrasounds are repeated and again show no DVT. He was discharged from the clinic with no anticoagulation, and was advised to seek medical attention again if he developed symptoms of DVT or PE.
- 1.Carrier M, Klok FA. Symptomatic subsegmental pulmonary embolism: to treat or not to treat? Hematology. Published online December 8, 2017:237-241. doi:10.1182/asheducation-2017.1.237
- 2.Long B, Koyfman A. Best Clinical Practice: Current Controversies in Pulmonary Embolism Imaging and Treatment of Subsegmental Thromboembolic Disease. The Journal of Emergency Medicine. Published online February 2017:184-193. doi:10.1016/j.jemermed.2016.08.021
- 3.Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease. Chest. Published online February 2016:315-352. doi:10.1016/j.chest.2015.11.026
- 4.Carrier M. A Study to Evaluate the Safety of Withholding Anticoagulation in Patients With Subsegmental PE Who Have a Negative Serial Bilateral Lower Extremity Ultrasound (SSPE). U.S National Library of Medicine Clinical Trials.gov. https://clinicaltrials.gov/ct2/show/NCT01455818
- 5.Righini M, Sanchez O, Roy P-M, et al. A positive compression ultrasonography of the lower limb veins is highly predictive of pulmonary embolism on computed tomography in suspected patients. Thromb Haemost. Published online 2006:963-966. doi:10.1160/th06-03-0158
All the content from the Blood & Clots series can be found here.
This post was reviewed by Brent Thoma, Sadad Rahman and copyedited by Rebecca Dang.

Carolyne Elbaz
Latest posts by Carolyne Elbaz (see all)
Eric Tseng
Latest posts by Eric Tseng (see all)
- Blood & Clots Series: Subsegmental PE – To Treat or Not To Treat? - June 25, 2020
- Blood & Clots Series: Is Fecal Occult Blood Testing helpful in deciding whether it’s safe to prescribe anticoagulants? - April 30, 2019
- Blood & Clots Series: How do I manage acute VTE in pregnancy? - September 25, 2018