
There are few things in ECG interpretation more irritating to a junior learner than fascicular blocks. You might find yourself asking whether the pattern is qR. Or maybe it’s rO. sO? ss? And what are these fascicle things anyway? (Figure 1)

Figure 1: Stylized schematic of the anterior and posterior fascicles of the heart. Note the relative widths of the anterior vs. posterior fascicles.
In this article, we will briefly explore the physiology of cardiac depolarization, with and without fascicular blocks. Then we get to the important stuff: how to recognize these syndromes on ECG, and how to treat them in the emergency department.
Objectives
- Review normal cardiac depolarization
- Review depolarization in fascicular blocks
- Learn a helpful mnemonic
- Discuss multi-fascicular blocks
- Consider treatments:
- Chemical
- Electrical
- Disposition
Normal Ventricular Depolarization and the Cardiac Axis
The term cardiac axis refers to the net cardiac vector, which is the summation of all of the tiny vectors that make up the cardiac depolarization wave. In reality, depolarization starts in many places simultaneously, and these individual depolarization waves sum together to form a net left-to-right septal vector [1].
In the normal heart, net depolarization begins at the septum and proceeds left-to-right across this structure. The depolarization then spreads down toward the apex of the heart. Finally, depolarization spreads back up to the walls of the ventricles (Figure 2) [1]. Since, in the normal heart, there is more myocardial mass to depolarize in the left ventricle than in the right, the cardiac axis on ECG ends up pointing left, between 0 and +90 degrees.

Figure 2: Normal cardiac depolarization
Left Anterior Superior Fascicular Block
Disease of the left anterior-superior fascicle (LASF) is the most common disorder of the fascicles. The left superior anterior fascicle is anatomically narrow, like a single conducting wire. It is supplied by the left anterior descending (LAD) artery, and its narrowness and vulnerable blood supply make it susceptible to ischemic damage [2, 3, 4]. When an LASF block exists, depolarization no longer begins in the septum, but instead at the endocardial surface of the inferoseptal wall of the heart via the posterior-inferior fascicle (LPIF). The depolarization wave spreads towards the epicardium first, which creates a small positive deflection in the inferior leads (Figure 3) [2].

Figure 3: Cardiac depolarization with a blocked LASF, part 1
Depolarization then proceeds upward towards the base of the heart, and left (where there is more myocardium). This produces a large negative deflection in the inferior leads, and a corresponding positive deflection in the lateral leads (Figure 4).

Figure 4: Cardiac depolarization with a blocked LASF, part 2
The changes to depolarization caused by the block result in a characteristic leftward axis on ECG (Figure 5). Other causes, such as LVH, must also be ruled out.
![Figure 5: LASFB ECG pattern [2]](https://canadiem.org/wp-content/uploads/2015/07/Figure-5.jpg)
Figure 5: LASFB ECG pattern [2]
- Endo-to-epicardial depolarization of the inferior wall — rS pattern in the inferior leads, qR pattern in the lateral leads
- Depolarization in an ‘up-and-left’ direction — Left-axis deviation
- Depolarization reaches left side of heart more slowly — Prolonged R-wave peak time in aVL
Left Posterior Inferior Fascicular Block
The physiology of the LPIF block is similar to that of LASF block. This type of block is much less common than LASF block, as this fascicle is a broad “fan” of conducting tissue, like a broad cable to the anterior superior fascicle’s thin wire. It is less susceptible to vascular injury from a single infarct [4, 5, 6].
Depolarization is initiated by the LASF at the endocardial surface of the anterolateral free wall, and spreads superiorly and leftwards, toward the epicardium (Figure 6) [5].

Figure 6: Cardiac depolarization with a blocked LPIF, part 1
At this point, the left side of the heart is mostly depolarized. Depolarization proceeds to the right, resulting in large S-waves in the lateral leads, and right axis deviation (Figure 7).

Figure 7: Cardiac depolarization with a blocked LPIF, part 1
Again, the ECG findings (Figure 8) follow from the physiology:
![Figure 8: LPIFB ECG pattern [5]](https://canadiem.org/wp-content/uploads/2015/07/Figure-8.jpg)
Figure 8: LPIFB ECG pattern [5]
- Endo-to-epicardial lateral wall depolarization —qR pattern in the inferior leads, rS pattern in the lateral leads
- Depolarization in a ‘rightward’ direction —Right-axis deviation
- Depolarization reaches right side of heart more slowly —Prolonged R-wave peak time in aVR
There are other diseases that cause right-axis deviation, such as right ventricular hypertrophy, pulmonary embolism, COPD, and Wolff-Parkinson-White syndrome. LPIFB cannot be diagnosed until other causes of right-axis deviation are ruled out [5, 6].
A Helpful Mnemonic
You may have noticed the emphasis on superior and inferior in the terms Left Anterior Superior Fascicle and Left Posterior Inferior Fascicle. This makes anatomical sense, as the anterior surface of the heart is superior to the posterior surface, but the reason for the renaming is mostly to set up a useful mnemonic: the direction of the initial deflection in the inferior ECG leads is the same as the name of the block. Since the lateral leads show the opposite morphology, this gives you both patterns!
For example, a left anterior superior fascicular block will produce an ECG with an initially positive (superior) deflection in the inferior leads: an rS pattern (Figure 9).

Figure 9: LASFB shows an initially superior deflection in the inferior leads
Conversely, a left posterior inferior fascicular block will show up as an initially negative (inferior) deflection in the inferior leads: a qR pattern (Figure 10). Remember that these initial deflections represent depolarization spreading from the endocardium to the epicardium.
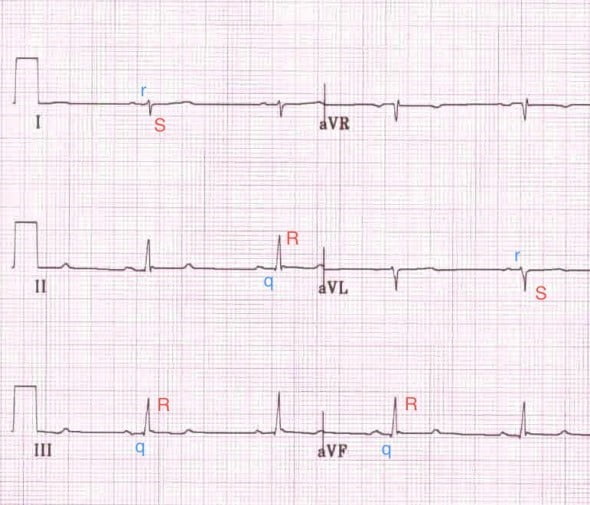
Figure 10: LPIFB shows an initially inferior deflection in the inferior leads
The second important ECG criteria for fascicular blocks is the axis deviation. The same trick works here: an anterior superior block has an axis deviation in the upper (superior) part of the Cabrera circle (Figure 11).
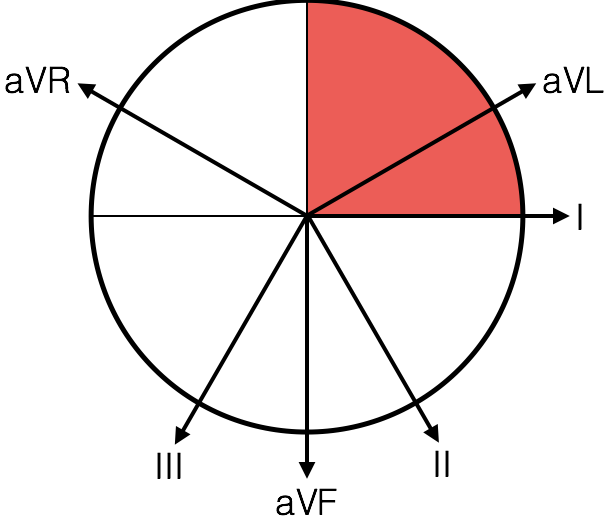
Figure 11: LASFB results in an axis in the superior quadrant
The posterior inferior block has an axis deviation in the lower (inferior) part of the circle (Figure 12).

Figure 12: LPIFB results in an axis in the inferior quadrant
Multifascicular Blocks
Ventricular conduction blocks can be described in terms of the number of fascicles that are affected: monofascicular, bifascicular, or trifascicular.
Monofascicular blocks are the syndromes described above in isolation; a single fascicle is damaged, but there is still conduction from the atria to the ventricles. This includes solitary LASFB, LPIFB, and right bundle branch block. Isolated monofascicular blocks are benign and require no treatment [7].
A bifascicular block occurs when two fascicles are impaired. The three possibilities are a LASFB and a RBBB, a LPIFB and a RBBB, or a left bundle branch block (as this is impairment of both the LPIF and LASF) [4]. These are normally well-tolerated and do not require treatment beyond avoiding AV-node-blocking medications if asymptomatic. In the case where the sole remaining fascicle is unhealthy or partially damaged, a Mobitz II block can occur; this is called an incomplete trifascicular block [8, 9]. This (infra-His) block often presents as a bifascicular block with a history of syncope, indicating transient complete block, and is a Class I indication for permanent pacing [7, 9]. Similarly, a fixed RBBB with separate ECGs demonstrating disease of both the LASF and LPIF is considered an alternating trifascicular block, and is also a Class I indication for permanent pacing [7]. Bifascicular blocks that coexist with a 1st degree AV node block are complicated and should be seen by cardiology. If the patient has experienced symptoms, such as syncope, they should be paced; asymptomatic individuals need not be paced [7].
![Figure 13: Bifascicular block – RBBB + LASFB (rS morphology inferiorly and left-axis deviation) [8]](https://canadiem.org/wp-content/uploads/2015/07/Figure-13.jpg)
Figure 13: Bifascicular block – RBBB + LASFB (rS morphology inferiorly and left-axis deviation) [8]
![Figure 14: Complete trifascicular block – RBBB + LASFB + A-V dissociation [10]](https://canadiem.org/wp-content/uploads/2015/07/Figure-14.jpg)
Figure 14: Complete trifascicular block – RBBB + LASFB + A-V dissociation [10]
Treatment Considerations
Chemical
As laid out in ACLS guidelines, many symptomatic bradycardias are treated with atropine. This medication can decrease AV-node blockade (and hence increase heart rate) by decreasing vagal tone. They reduce the vagal nerve’s inhibition of the AV node, and increase the SA nodal rate. In the case of a complete trifascicular block (or an incomplete block such as a Mobitz II), the blocking lesion is distal to the AV node, and atropine in unlikely to have any effect. While atropine is unlikely to cause harm, its lack of efficacy in patients with an acute bradycardia resulting from a trifascicular block means that its use should be avoided in favour of cardiac pacing [11].
Electrical
In an unstable patient with a trifascicular block, the most effective option for restoring hemodynamic stability is with electricity. Transcutaneous and transvenous pacing causes the ventricle to beat at a rate of our choosing — one more compatible with life!
Disposition
A new, isolated fascicular block is benign and not uncommon, but should prompt investigation for the underlying cause, which is most often ischemia.
New, asymptomatic bifascicular blocks do not need urgent management (though reversible causes should be ruled out), and should be referred to cardiology. Avoid any medications that impair the AV node.
Patients with bifascicular block and a 1st degree heart block technically have an incomplete trifascicular block. They may not require pacing if asymptomatic, but they do warrant further work-up [4, 7, 10]. They should be referred to cardiology and have their medications reviewed for any AV-node impairing agents.
People on transvenous pacing can’t go home until they have had their pacer “internalized”, so patients who have been paced will need to see an electrophysiologist. Patients with a new incomplete trifascicular block also need to see an electrophysiologist for pacemaker implantation
Conclusion
The anatomy of the cardiac fascicles is complicated. As emergency room physicians, we need to recognize fascicular blocks on ECG, and implement pacing as therapy for symptomatic bradycardia caused by a trifascicular block,. Patients with new complete trifascicular blocks or incomplete trifascicular blocks (such as a Mobitz II pattern) need urgent referral to an electrophysiologist for pacemaker implantation.
[bg_faq_start]References
- Guyton AC, Hall JE. Guyton and Hall Textbook of Medical Physiology. Philadelphia: Saunders Elsevier; 2011.
- Burns E. Left Anterior Fascicular Block. Life in the Fast Lane ECG Library. Available at: http://lifeinthefastlane.com/ecg-library/basics/left-anterior-fascicular-block/. Accessed March 26, 2015.
- Sauer WH. Left anterior fascicular block. UpToDate. November 04, 2013. Available at: http://www.uptodate.com/contents/left-anterior-fascicular-block. Accessed March 26, 2015.
- Piktel JS. Cardiac Rhythm Disturbances. In: Tintinalli JE, ed. Tintinalli’s Emergency Medicine. Seventh Edition ed. New York: McGraw-Hill; 2011.
- Burns E. Left Posterior Fascicular Block. Life in the Fastlane ECG Library. Available at: http://lifeinthefastlane.com/ecg-library/basics/left-posterior-fascicular-block/. Accessed March 26, 2015.
- Sauer WH. Left posterior fascicular block. UpToDate. November 04, 2013. Available at: http://www.uptodate.com/contents/left-posterior-fascicular-block. Accessed March 26, 2015.
- Epstein AE, DiMarco JP, Ellenbogen KA, Estes NA, Freedman RA. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. May 2008;117(21):e350-408.
- Burns E. Bifascicular Block. Life in the Fastlane ECG Library. Available at: http://lifeinthefastlane.com/ecg-library/basics/bifascicular-block/. Accessed March 26, 2015.
- Sauer WH. Course and treatment of chronic bifascicular block. UpToDate. January 17, 2014. Available at: http://www.uptodate.com/contents/course-and-treatment-of-chronic-bifascicular-block. Accessed March 26, 2015.
- Burns E. Trifascicular Block. Life in the Fastlane ECG Library. Available at: http://lifeinthefastlane.com/ecg-library/trifascicular-block/. Accessed March 26, 2015.
- Neumar RW, Otto CW, Link MS, Kronick SL, Shushter M, Callaway CW. Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(suppl 3):S729-S767.

Tristan Jones
Latest posts by Tristan Jones (see all)
- CRACKCast E190 – Disaster Preparedness - June 28, 2018
- CRACKCast Episode 142 – Electrical and Lightning Injuries - January 8, 2018
- CRACKCast E133 – Parasitic Infections - December 7, 2017
Latest posts by BoringEM (see all)
- Pre-Game: CaRMS Interview Preparation - December 20, 2017
- Tiny Tips: SALTR for Pediatric Growth-plate Fractures - May 20, 2016
- Does that condition require investigation? - May 10, 2016