
This 123rd episode of CRACKCast covers Rosen’s 9th edition, Chapter 115, Selected Oncologic Emergencies. With an ever aging population, cancer incidence continues to rise. Therapies continue to prolong life often with high risks of side effects, and emergency physicians need to be equipped to treat complications of this treatment and importantly cancer morbidity itself.
Shownotes – PDF Here
Also check out EMCases Rapid Review on Oncologic Emergencies Part 1 and Part 2
[bg_faq_start]Key Concepts
- Patients whose absolute neutrophil count is or is expected to soon be 500 cells/mm3 or less are considered severely neutropenic. A single temperature of 38.3°C or sustained temperature of 38.0°C for at least 1 to 2 hours is considered fever.
- Any neutropenic patient with fever or with infectious signs or symptoms (even in the absence of fever) should be worked up for an infectious source, including drawing of blood cultures, and started on empirical antibiotics. Those with high-risk features (eg, prolonged or profound neutropenia, pneumonia, hypotension, abdominal pain, neurologic changes, MASCC score <21) should be started on an antipseudomonal beta-lactam (eg, cefepime, piperacillin-tazobactam, antipseudomonal carbapenem). Those with low-risk features may be appropriate for oral antibiotics. Empirical gram-positive bacterial, antifungal, and antiviral coverage is unnecessary unless the clinical situation dictates otherwise.
- Neutropenic patients with fever should generally be hospitalized, including all high-risk patients. Select low-risk patients may be managed as outpatients.
- Vertebral metastasis and spinal cord compression should be considered in any patient, particularly those with known cancer who have back pain, peripheral strength or sensory loss, or loss of bowel or bladder function.
- MRI of the spine is the preferred diagnostic test when evaluating spinal cord compression. CT of the spine with myelography may be performed if MRI is contraindicated or unavailable. Plain films are not sufficiently sensitive to rule out spinal cord compression.
- Intravenous corticosteroids (dexamethasone 10 mg bolus) should be given to any patient with neurological deficits from known or suspected metastatic spinal cord compression. Consideration should be given to emergent surgical and radiation treatment if compatible with goals of care.
- Cardiac tamponade occurs when pericardial pressures inhibit cardiac filling and output. No clinical sign or symptom is entirely sensitive for cardiac tamponade, but echocardiogram findings of large pericardial effusion (anechoic stripe around the heart), and atrial or right ventricular collapse during diastole, combined with clinical findings of shock are highly suggestive.
- If compatible with goals of care, pericardial effusion causing tamponade should be emergently drained. Intravenous fluid or inotrope administration may be trialed as a temporizing measure, but these therapies are unreliable and should not delay definitive management.
- Calcium levels in hypercalcemic patients should be assessed by measuring ionized calcium concentration, rather than total calcium concentration.
- First-line management of hypercalcemia includes intravenous fluids, and loop diuretics only for volume management, as well as bisphosphate therapy (pamidronate 90 mg or zoledronate 4 mg, intravenously). Calcitonin is faster acting than bisphosphonates, but tachyphylaxis may develop; consider calcitonin in hypercalcemic patients with active cardiac or neurologic symptoms (eg, dysrhythmias, seizures).
- TLS is manifested by the combination of hyperkalemia, hyperuricemia, hyperphosphatemia, and hypocalcemia, often accompanied by acute renal failure.
- Patients with TLS should have their potassium, phosphate, calcium, and uric acid levels, as well as renal indices monitored closely. Intravenous fluids should be administered, as well as therapies to reverse hyperkalemia. Hyperuricemia may be prevented with allopurinol or treated with rasburicase. Calcium should only be repleted in patients with cardiac or neurologic manifestations of hypocalcemia.
- Leukostasis arises due to congestion of blood vessels by excessive numbers of leukocytes. This most often occurs in the lungs and CNS, and the resulting clinical picture may be difficult to differentiate from other diseases which afflict cancer patients (eg, pneumonia, pulmonary embolism, CNS hemorrhage).
- In leukostasis, intravenous fluids should be administered in the ED to reduce blood viscosity, and red blood cell transfusions should generally be avoided. Therapies to lower the WBC count should be performed in consultation with an oncologist, and may include leukapheresis, administration of hydroxyurea, or initiation of chemotherapy.
- SVC syndrome occurs due to either external (eg, tumor) or internal (eg, thrombus) obstruction of the SVC.
- ED management of SVC syndrome is largely supportive. The head of the bed should be elevated and supplemental oxygen provided if needed. If the cause of SVC syndrome is determined to be thrombus, anticoagulation may be initiated if not contraindicated.
- SVC syndrome is life threatening in the rare case of cerebral edema, hemodynamic collapse, or tracheal compromise. Definitive anti-cancer treatment should be postponed to allow for tissue diagnosis of the underlying mass if not already known.
Rosen’s in Perspective
- “In 2010, about six hundred thousand Americans, and more than 7 million humans around the world, will die of cancer. In the United States, one in three women and one in two men will develop cancer during their lifetime. A quarter of all American deaths, and about 15 percent of all deaths worldwide, will be attributed to cancer. In some nations, cancer will surpass heart disease to become the most common cause of death.” – Siddhartha Mukherjee, The Emperor of all Maladies
- Cancer is only expected to become more common as the population continues to age.
- In the ED, we must be prepared to manage cancer patients and their complications.
- We also know there is a Knowledge Translation gap in managing oncologic emergencies in the ED. One recent study showed EPs have low rates of adherence to guidelines for low-risk febrile neutropenia patients, and tended to over treat and over admit, exposing patients to unnecessary risk and at an unnecessary cost to the system (Baugh et al., Acad Emerg Med 2017;24(1):83-91).
[1] List 5 causes of fever in the cancer patient
- Infection* (only identified in ⅓ of patients)
- DVT / Pulmonary embolus
- Chemotherapy or medication effect
- Direct tumor burden effect
- Transfusion reaction
For those presenting with bacterial infection, 30% of these patients will be bacteremic at time of presentation. Many of these patients will not mount the immune response needed for the typical symptoms and signs of infection. Infection is most important diagnosis to rule out, but other diagnoses should be considered.
[2] What is the definition of neutropenia? Febrile neutropenia?
- Neutropenia
- i) Neutrophils have shortest half life of all cell lines.
- ii) Risk of infection increases when ANC <1000, and greatly increases when ANC <500. Risk increases with prolonged neutropenia.
- Historical definition: ANC 1000-1500 is mild, 500-1000 is moderate, <500 is severe.
- Febrile neutropenia needs two components:
- i) Febrile: single T of 38.3 or sustained 38.0 for ≥1 hour
- ii) Neutropenia: absolute neutrophil count <500 cells/mm3 or expected to drop below this threshold within 48h
- WBC nadir happens about 3-14 days after chemo
- However, any neutropenic patient with signs and symptoms of infection should be treated as having neutropenic fever as the mortality is ~20%.
[3] What are the most common infections in febrile neutropenia?
- Most common infections: pneumonia, anorectal lesion, skin infection, pharyngitis, UTI
- i) Expert opinion: against DRE to prevent compromising blood/rectal barrier (also, unlikely to gain any useful information)
- ii) Examine mucous membranes, dermatological exam including anorectal area, indwelling lines, head/neck area for sinusitis
[4] What are high risk and low risk criteria for febrile neutropenia?
- Scoring systems
- MASCC or CISNE scoring systems
- A recent retrospective cohort study by Coyne et al. (Ann Emerg Med 2017;69(6):755-764) showed CISNE has higher specificity for identifying low risk patients who can be managed with oral antibiotics and close f/u within 2-3 days to recheck fever and neutrophil count (98% vs 54% specificity)
- MASCC or CISNE scoring systems
| MASCC | CISNE |
| Symptom severity / burden of illness Hypotension BP<90 COPD Type of Cancer Dehydration Outpatient vs inpatient Age>60 | ECOG Performance status Stress induced hyperglycemia COPD Cardiovascular disease Hx Severe mucositis Monocytes <200/uL |
Other general criteria to consider (Combo of BC Cancer Agency, IDSA)
- Host factors
- Age >60-70
- Comorbidities
- Inpatient status at time of fever
- Poor performance status
- Disease factors
- Hemodynamic instability
- Anticipated prolonged profound neutropenia (ANC <0.1 x 10^9 for >7 days)
- Renal insufficiency (Serum Cr >176)
- Hepatic insufficiency LFT 3-5x ULN
- Uncontrolled, progressive CA
- Severe mucositis that interferes with swallowing or causing severe diarrhea
- GI symptoms – abdominal pain, N/V, diarrhea
- Neurologic or mental status changes of new onset
- New pulmonary infiltrate, hypoxemia or underlying chronic lung disease
- Indwelling catheter
[5] What is the empiric treatment of febrile neutropenia?
- Workup – sepsis workup including blood cultures
- 1 off central line if existing
- Empiric broad spectrum antibiotics (no time frame in IDSA guidelines, but recommended to start after BC drawn)
- Consult oncology – almost all will be admitted; if they are unstable they get admitted to ICU
- CXR not routinely recommended unless respiratory symptoms
- Empiric treatment
- Broad spectrum Gram Positive and Gram Negative coverage, including Pseudomonas
| Low Risk | High risk | |
| – Oral ciprofloxacin (high dose 750 q12h) – Oral amox/clav | Empiric therapy | Broad spectrum with anti-pseudomonal coverage
-Pip Tazo -4th Gen Cephalosporin (Cefipime) or Ceftazidime -Meropenem or Imipenem (also covers ESBL) -Fluoroquinolone -Aminoglycosides |
| -Oral Ciprofloxacin -Oral Clindamycin | True Penicillin allergy | -Vancomycin -Aminoglycoside -Ciprofloxacin |
[6] In addition to empiric therapies, which patients with febrile neutropenia should receive additional antibiotic coverage?
| Vancomycin IDSA 2010 Guidelines + BC Cancer Agency | 1) Hemodynamic instability / Sepsis 2) Pneumonia 3) +BC for G+ cocci 4) SSTI 5) MRSA known or suspected 6) Severe mucositis |
| Ciprofloxacin (or aminoglycoside) BC Cancer Agency | 1) Resistance suspected 2) Hypotension 3) Persistent fever 4) Pneumonia |
| Metronidazole BC Cancer Agency | Suspicion of anaerobic infection (e.g., intra-abdominal) |
| Acyclovir Rosen’s 9th Ed | 1) Herpetic lesions 2) Encephalopathy |
| Antifungal IDSA 2010 Guidelines + BC Cancer Agency | Persistent fevers despite receiving 3-5 (BCCA) or 4-7 days (IDSA) days of broad spectrum antibiotics with anticipated duration of neutropenia >7 days |
| Risk of Pneumocystis jirovecii Pneumonia UpToDate | 1) Acute Lymphocytic Leukemia 2) CNS tumors 3) Other cancer patients receiving high dose corticosteroids |
Therefore, a patient with febrile neutropenia in true septic shock in a coma with a distended abdomen should receive a regimen like Meropenem, Vancomycin, Ciprofloxacin, Acyclovir +/- Metronidazole. Would definitely want your ID consultants involved in a (rare) case like this!
N.B., the above recommendations are a compilation of the IDSA 2010 Guidelines, the BC Cancer Agency Guidelines, Rosen’s 9th Ed, and UpToDate. Local resistance patterns and local guidelines should always be taken into account when choosing antibiotic therapies.
[7] What are the signs and symptoms of spinal cord compression? How is it treated?
- Signs / Symptoms
- Back pain (95%)
- Weakness
- Sensory loss / Saddle anesthesia
- Autonomic dysfunction (bowel/bladder dysfunction – late finding)
- Treatment
- Dexamethasone 10 mg IV then 16 mg po in divided doses daily
- Temporizes vasogenic edema
- Paraplegia may require much higher doses; No neurologic deficits may require no steroid
- Radiation vs. Surgery; Surgical Decompression then Radiation often done
- Definitive therapy within 24 h
- Best prognostic marker is initial neurological status
- Hospitalize if neurologic deficit
- Dexamethasone 10 mg IV then 16 mg po in divided doses daily
Some considerations for Radiation vs. Surgery include surgical vs nonsurgical candidate, single level vs multilevel.
[8] List 4 causes of pericardial effusion in the cancer patient:
- Malignancy (lung, breast, hematologic, melanoma)
- Hypoalbuminemia
- Radiation
- Chemotherapy
Something to consider in any cancer patient presenting with dyspnea or chest pain! (Affect >10% of cancer patients). Speed of accumulation is more important than strict volume.
[9] List 3 electrocardiographic and 3 echocardiographic findings of tamponade
- EKG:
- Low voltage
- Sensitive definition: QRS amplitudes in I + II + III < 15mm OR QRS amplitudes in V1+ V2 + V3 < 30mm
- Specific definition: Limb leads (I, II, III, aVR, aVF, aVL) all <5mm OR Precordial leads all <10mm
- Tachycardia
- Electrical alternans (10% of cases)
- Low voltage
- Echo
- RV diastolic collapse
- RA systolic collapse
- IVC dilation (no respiratory variation or collapse)
- Sonographic alternans
Best echo views are subcostal views (most sensitive) and apical views. It should be noted that the echo criteria are somewhat subjective. The RA systolic collapse is actually more sensitive than RV diastolic collapse as the RA is a thinner walled structure. To distinguish systole from diastole, M Mode can be used. Find the E and A waves of the mitral valve, which is when the mitral valve opens. This represents diastole. This can then be correlated to the RV free wall and seeing whether there is a “dip” which represents collapse of the RV during diastole. This may be hard to visualize, so check out the Ultrasound Podcast video lecture on this!
[10] Describe the presentation and management of hypercalcemia.
- Presentation
- Nonspecific presentation
- Stones – Nephrolithiasis
- Bones – Bony pain, pathological fracture
- Abdominal Groans – Anorexia, Consiptation, Abdominal Pain
- Psychiatric Moans – Altered LOC (depression, delirium)
- Calcium levels (generally above 3 mmol/L to cause symptoms, >3.5 mmol/L to cause severe symptoms)
- Can use ionized calcium if concerned about low albumin (e.g., malnourished) or high serum protein (e.g., Multiple Myeloma)
- EKG: Shortened QT Interval <350 ms
- Nonspecific presentation
Hypercalcemia secondary to malignancy signifies advanced disease with a median survival of 2 months.
- Management
- Dilution
- First line: IVF 200-500 cc/h
- Fluid challenge recommended for oliguric/anuric patients
- Loop diuretics – PRN only for volume management
- Thiazides will make hypercalcemia worse
- Dialysis – PRN only for refractory hypercalcemia / volume overload
- First line: IVF 200-500 cc/h
- Osteoclast inhibition
- Calcitonin – PRN only for cardiac dysrhythmias or seizures
- Susceptible to tachyphylaxis
- Bisphosphonate
- Pamidronate 90 mg IV or Zoledronate 4 mg
- Take days to work – inpatient management
- Caution in renal impairment
- iii) ?Decreased calcitriol production
- Glucocorticoids (e.g., Prednisone)
- Calcitonin – PRN only for cardiac dysrhythmias or seizures
- Dilution
[11] What are the typical electrolyte abnormalities associated with tumour lysis syndrome? What are the risk factors for tumour lysis syndrome? What are the potential complications?
- Electrolyte abnormalities resulting from intracellular release of massive malignant cell lysis
- Hyperkalemia (cell cytosol)
- Hyperuricemia (DNA breakdown)
- Hyperphosphatemia (protein breakdown)
- Hypocalcemia
- Results from free calcium precipitating with excess phosphate → calcium phosphate crystal deposition in kidney
- Risk factors
- Tumor factors
- High burden, rapidly growing, highly chemosensitive
- g., ALL, Burkitt’s lymphoma
- Undergoing cytotoxic therapy
- High burden, rapidly growing, highly chemosensitive
- Patient factors
- Preexisting renal failure
- Hypovolemia
- Hyperuricemia
- Tumor factors
- Complications
- Nephrotoxicity / AKI – exacerbates electrolyte abnormalities
- Calcium phosphate crystal deposition
- Urate nephropathy
- +/- Xanthine crystal deposition
- Nephrotoxicity / AKI – exacerbates electrolyte abnormalities
[12] Describe 4 treatments for Tumor Lysis Syndrome
- IVF 5-6 L/day
- i) Oliguric/anuric patients may need renal replacement therapy
- Hyperkalemia treatments/shifting
- i) Calcium only if cardiac, neuro issues
- Hyperuricemia treatment
- i) Allopurinol (prevents conversion xanthine –> uric acid, does not eliminate existing uric acid)
- ii) Rasburicase (direct elimination)
- Hypocalcemia treatment
- i) IV Calcium only if cardiac or neurological complications
[13] What is Leukostasis? How does it present?
- Pathophysiology
- WBC high enough to cause vascular congestion, particularly in lungs or CNS (no specific WBC threshold), most often occurs in pulmonary or central nervous systems.
- Associated with leukemias (AML, CLL)
- Clinical presentation
- Nonspecific symptoms
- Pulmonary leukostasis presents like PNA or pulmonary edema
- Dyspnea, Tachypnea, Hypoxemia
- CNS leukostasis presents with altered LOC
- Confusion, audio/visual abnormalities, h/a, ataxia, coma
- Pulmonary leukostasis presents like PNA or pulmonary edema
- Nonspecific symptoms
[14] Which conditions are associated with hyperviscosity syndrome? What is the classic clinical triad?
- Causes of hyperviscosity syndrome
- Elevation of cellular contents of blood (leukostasis, polycythemia)
- Cryoglobulinemic Hyperviscosity (e.g., Multiple Myeloma)
- Increased viscosity due to polyclonal or monoclonal immunoglobulins that are not cryoglobulins (e.g., Waldenstrom’s macroglobulinemia)
- Partial obstruction by sickled RBCs
- Partial obstructed by parasitized cells (malaria, Babeiosis)
- Clinical Presentation
- Mucosal bleeding (epistaxis, hematuria, vaginal/rectal bleeding)
- Visual disturbances
- Altered LOC
No practical diagnostic test for hyperviscosity syndrome; clinical diagnosis. In hyperviscosity syndrome, the mucosal bleeding is seen when myeloma proteins (e.g., in patients with multiple myeloma) interfere with platelet function. The other symptoms of HVS are due to sludging effects.
[15] Describe the clinical presentation of superior vena cava syndrome.
- Results from external or internal compression of the SVC
- Upper extremity, chest or face edema or erythema
- +/- dyspnea, chest pain, cough
- Physical exam shows elevated venous return pressures – e.g., JVD, cyanosis to upper trunk
- Can attempt Pemberton’s sign: facial redness caused by elevating the arms above the head
- Vein collaterals could signify subacute disease process
- Edema and flushing isolated to upper body with history of lung cancer or lymphoma is highly suspicious for SVC syndrome
The vast majority of these patients have slowly developing processes and are stable in the short term. Biopsy specimens can often be done before treatment.
[bg_faq_end]WiseCracks
[bg_faq_start][1] Describe the key parts of calcium homeostasis
Figure 115.4
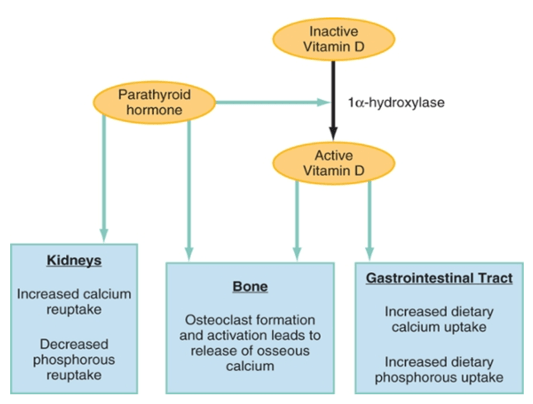
- *Active Vitamin D is also called Calcitriol
- Oncologic patients get hypercalcemia via the following mechanisms:
- PTHrP synthesis (80%)
- Calcitriol overproduction
- Bone osteolysis due to direct tumor spread
- Ectopic PTH production (rare)
[2] List common cancers that metastasize to bone
- P.T. Barnum Loves Most Kids.
- Prostate
- Testes
- Breasts
- Lungs
- Multiple Myeloma
- Kidney
[3] List 5 causes of SVC syndrome
- Malignancy (Lung cancer, Lymphoma)
- Thrombosis
- i) Intravascular devices (pacemaker, pacemaker leads)
- Fungal infections – Endocarditis (contiguous spread); Fibrosing mediastinitis (usually from excessive host response to previous Histoplasma infection)
- Postradiation fibrosis
- Bacterial infections – TB, syphilis
[4] List 5 cardiovascular complications of malignancy.
- SVC syndrome
- DVT/PE
- Cardiac dysrhythmias secondary to electrolyte disturbances (e.g., hyperkalemia)
- Malignant pericardial disease / tamponade
- Carotid blowout syndrome / carotid artery rupture
- Usually occurs in head and neck cancers with a surgically exposed carotid artery with limited residual overlying tissue (often secondary to radiation changes)
[5] List 6 neurological complications of malignancy.
- Spinal cord compression / cauda equina
- Electrolyte disturbances: Hypercalcemia; Hyponatriemia / SIADH
- Leukostasis / Hyperviscosity syndrome
- Brain metastasis
- Hydrocephalus
- Brain abscess / Meningitis / encephalitis
Other resources:
- EM Cases Episode 33: Oncologic Emergencies.
- IDSA 2010 Guidelines on Febrile Neutropenia.
- BC Cancer Agency Guidelines on Febrile Neutropenia.
Acknowledgements:
- Dr. Justin Ahn (Royal Columbian Hospital) for his guidance and feedback!
This post was uploaded and copyedited by Riley Golby (@RileyJGolby)

Adam Thomas
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018

Daniel Ting
Latest posts by Daniel Ting (see all)
- Dress for Success: A Guide to Dressing Choices for Common Wounds in the Emergency Department - April 25, 2024
- 2023 CanadiEM Year in Review and Editor’s Choice Awards - January 2, 2024
- Call for Junior Editors, Class of 2023-24 - September 21, 2023

Tristan Jones
Latest posts by Tristan Jones (see all)
- CRACKCast E190 – Disaster Preparedness - June 28, 2018
- CRACKCast Episode 142 – Electrical and Lightning Injuries - January 8, 2018
- CRACKCast E133 – Parasitic Infections - December 7, 2017