

This episode of CRACKCast covers Rosen’s Chapter 16, Depressed Consciousness and Coma. This presentation has a broad differential, but the systematic approach outlined here will guide your strategic work up for these altered patients.
Shownotes – PDF Link Here
[bg_faq_start]Rosen’s in Perspective
Depressed mental status represents an alteration in arousal stemming from a wide spectrum of diseases and presenting on a continuum of impairments. These impairments range from sleepiness, to decreased alertness, to coma. A common approach to this broad differential is DIMS, which is covered later in this episode.
Physiology
Consciousness is the awareness of one’s self or surroundings, and is composed of:
- Arousal – this is what we refer to as “altered” in altered level of consciousness
- Dynamic levels on a continuum:
Fully alert <-> Stuporous <-> Comatose <-> Complete unconsciousness
- Cognition – a composite of several factors leading to “states” of consciousness:
- Orientation – accurate perception of what is experienced
- Judgement – ability to process data in order to generate more meaningful info
- Memory – ability to store and retrieve information
- Many medical states can alter cognition (confusion, inattention, delusions, dementia) however, since these states do not depress level of arousal.
Pathophysiology
Arousal is controlled by the ascending reticular activating system (ARAS) in the paramedian tegmental zone of the dorsal brainstem
- Determines arousal and cortical activation
Cognition is primarily controlled by the cerebral cortex
- Determines content of consciousness
Therefore anything impacting normal function of the brainstem (small lesion = large deficit) or bilateral cortex can cause depressed consciousness or coma.
The three categories of processes that insult these anatomical areas include:
- Metabolic derangements
- Toxins
- Mechanical injury
1) List a broad differential diagnosis for coma
[bg_faq_start]DIMES Approach to Altered LOC
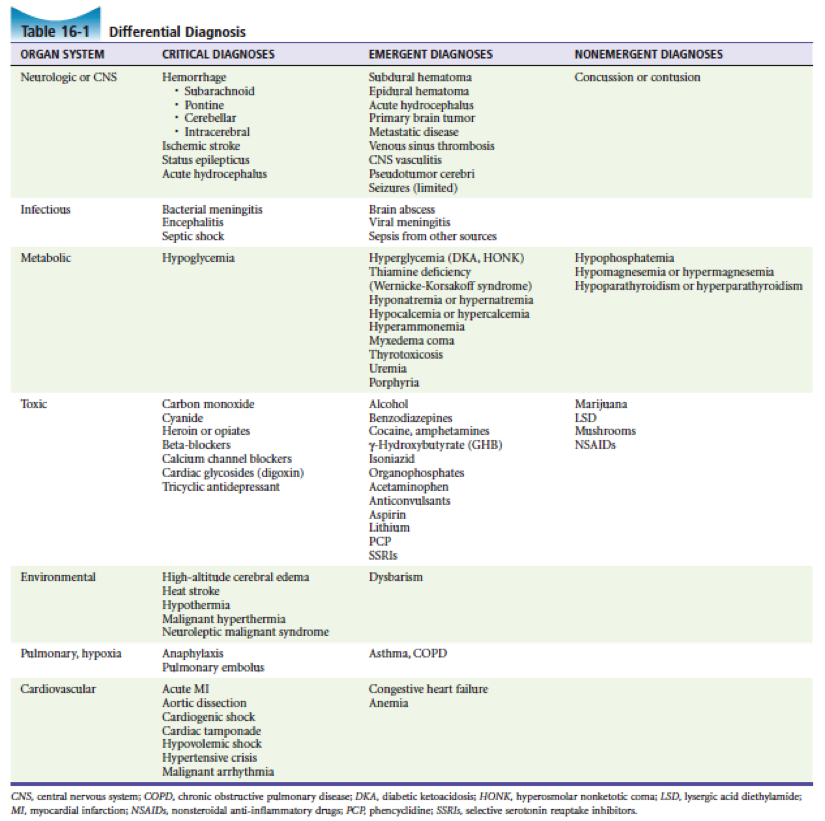
Break down of table 16-1: using the DIMES approach (“if you don’t think of it you’ll never dx it”)
[1] Drugs:
The “OB’s 5Cs” as the Critical diagnoses:
- Opiates
- Beta-blockers
- Carbon monoxide
- Cyanide
- CCBs
- Cyclic antidepressants
- Cardiac glycosides
- Abuse: heroin, opiates, benzodiazepines, alcohol, cocaine, amphetamines, marijuana, LSD, mushrooms, GHB
- Accidental: Carbon Monoxide / Cyanide
- Acquired: BB, CCBs, digoxin, TCAs, acetaminophen, ASA, SSRI, anticonvulsants
[2] Infection:
- Meningitis, encephalitis,
- Septic shock and sepsis
[3] Metabolic (by organ system)
- Pancreas
- Hypoglycemia
- DKA, HONK
- Thyroid (hyper or hypothyroid)
- Kidneys (electrolyte derangements, kidney failure with uremic state)
- Liver (hepatic encephalopathy)
[4] Environmental
- High altitude cerebral edema
- Heat stroke
- Hypothermia
- Dysbarism
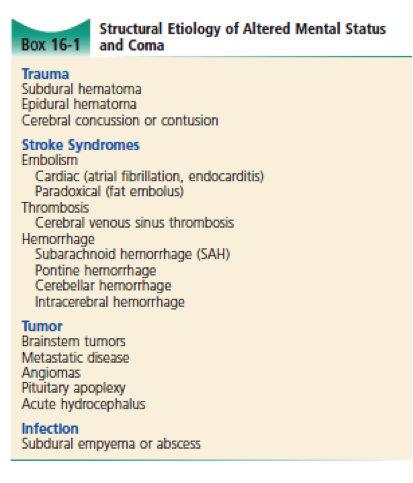
[5] Structural
- Intracranial Catastrophe
- ICH, Stroke, Epidural hematoma, Subdural hematoma, SAH
- Status epilepticus, acute hydrocephalus
- Cardiac
- ACS, Aortic Dissection
- Cardiogenic / Hypovolemic / Obstructive / Distributive shock
- HTN crisis, malignant arrhythmia
AEIOU TIPS Approach to Altered LOC
- Anaphylaxis or altitude illness or alcohol
- Epilepsy (pre, intra, or post ictal) or Environmental (hypo/hyperthermia or altitude)
- Infection
- Overdose of drugs (insulin, benzos, etc.)
- Underdose of drugs
- Trauma (TBI, hemorrhage) / Tumour
- Insulin
- Psychogenic / Poisons
- Stroke / Shock
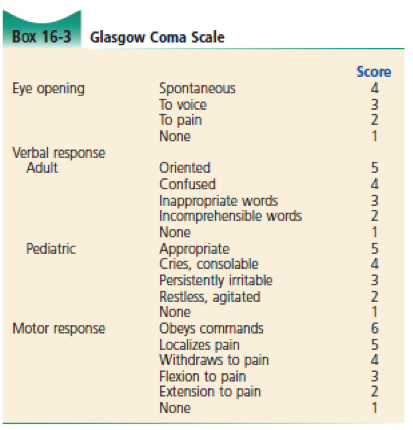
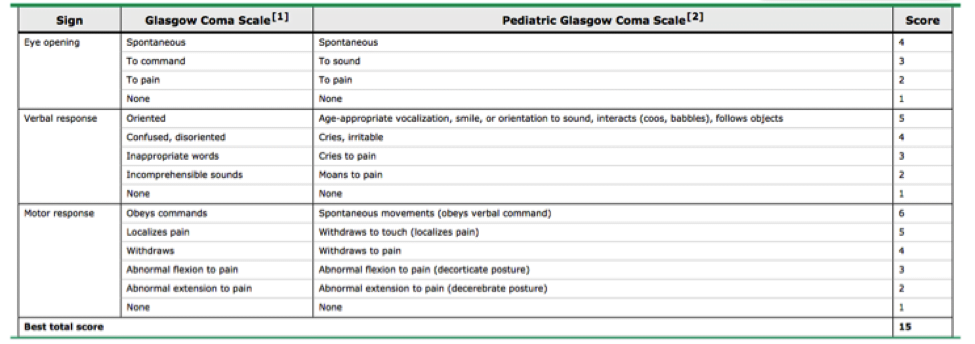
2) List GCS / Pediatric GCS
Need to know this!
- Glasgow Coma score <8 intubate.
- Remember change >2 points is significant change.
- Recent SMACC talk (Mark Wilson SMACC Chicago) discusses need to describe specifically what E, M and V are. See: http://www.smacc.net.au/2016/03/goodbye-gcs-mark-wilson/
Note that for Verbal Response:
- Adult and pediatric scoring varies
- “V” for 5 possible scores
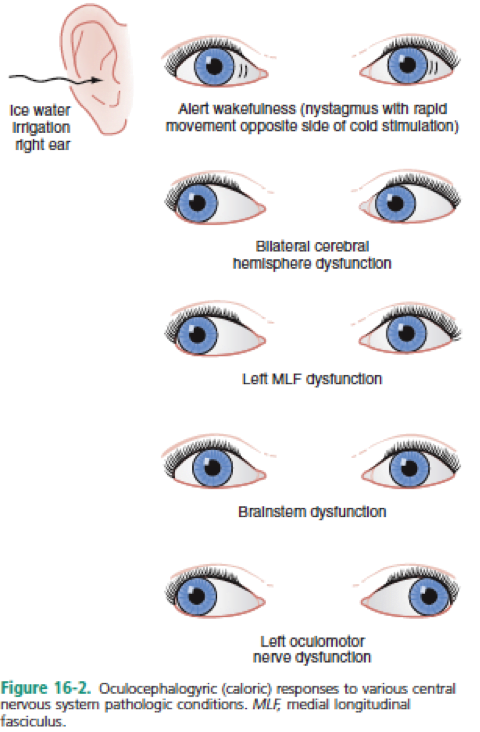
3) Describe the oculocephalic and oculovestibular reflex
Important tests, as if they give a normal response then a structural lesion in brainstem is unlikely
Oculo-Cephalic – Doll’s eyes.
Make sure no contraindications (mainly c-spine precautions)
- Observe eyes with moving head side to side (cervical rotation).
- If eyes remain fixed / frozen in orbits, this is an abnormal response
- If eyes maintain forward gaze despite turning the head, this is a positive doll’s eye reflex and is considered the normal response
Oculo-Vestibular – Cold Calorics.
Ensure no perforated tympanic membranes / Excessive earwax
- Elevate patient’s head 30 degrees OR reverse trendelenburg (if c-spine precautions)
- Instill 10-30cc of ice cold water into ear
REMEMBER COWS – Cold Opposite, Warm Same
- Referring to direction of nystagmus in relation to water
If there is an intact brainstem:
- Instilling cold water into right external auditory canal will result in slow conjugate deviation towards to the cold ear for 30-120 seconds, with fast nystagmus beats away from the cold ear.
If the brainstem is not intact:
- There will be no movement with irrigation.
Wise Cracks
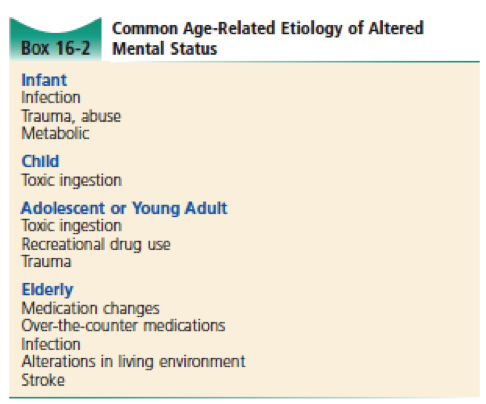
1) List the common age related causes of altered mental status
2) What is the initial management of an ALOC patient:
- Step 1: MOVIE (monitors, oxygen, vitals, IV, environment)
- Step 2: ABCs
- Step 2: Blood Sugar, Temp, ECG
- Step 3: Coma Cocktail: Dextrose, Oxygen, Narcan, Thiamine
- Step 4: CXR, CT Head, Consider antibiotics +/- antivirals, metabolic antidotes, Trauma management, secondary surveys
This post was uploaded and copyedited by Riley Golby (@RileyJGolby)
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018

Tristan Jones
Latest posts by Tristan Jones (see all)
- CRACKCast E190 – Disaster Preparedness - June 28, 2018
- CRACKCast Episode 142 – Electrical and Lightning Injuries - January 8, 2018
- CRACKCast E133 – Parasitic Infections - December 7, 2017