
A Case:
A 32-year-old female was the driver in a simple rear-end motor vehicle collision at about 40km/h. She was wearing a seatbelt and her airbags did not deploy. She extricated herself from the car. When EMS arrived, she was walking.
On examination by paramedics, the young woman denied paraesthesias. She did complain of midline C-spine tenderness; as a result, she was boarded and collared prior to transport.
She is now on a stretcher in your emergency department.
The Clinical Question:
Which clinical decision rule (Canadian C-spine vs. NEXUS) should you use to asses this patient?
The Analysis:
The Canadian C-Spine Rule (CCR) and the National Emergency X-Radiography Utilization Study Low-Risk Criteria (NEXUS criteria) are clinical decision tools developed to help us decide when blunt trauma patients require C-spine X-ray. The CCR was developed by Stiell and colleagues in 2001. Since then, the CCR has been validated for use in the emergency department, at triage, and by paramedics in the field. It uses 3 primary factors to determine whether a given patient needs imaging: 1) Is there any high-risk factor that mandates radiography? 2) Is there any low-risk factor that allows safe assessment of range of motion? 3) Can the patient actively rotate his or her neck 45° right and left? (See Figure 1) Strict exclusion criteria eliminate some of the ED population. (See Table 1)
| Figure 1. Canadian C-Spine Rules (Diagram has been re-designed by the BoringEM.org team for clarity – click on the diagram to link to a higher-resolution version of the picture) |
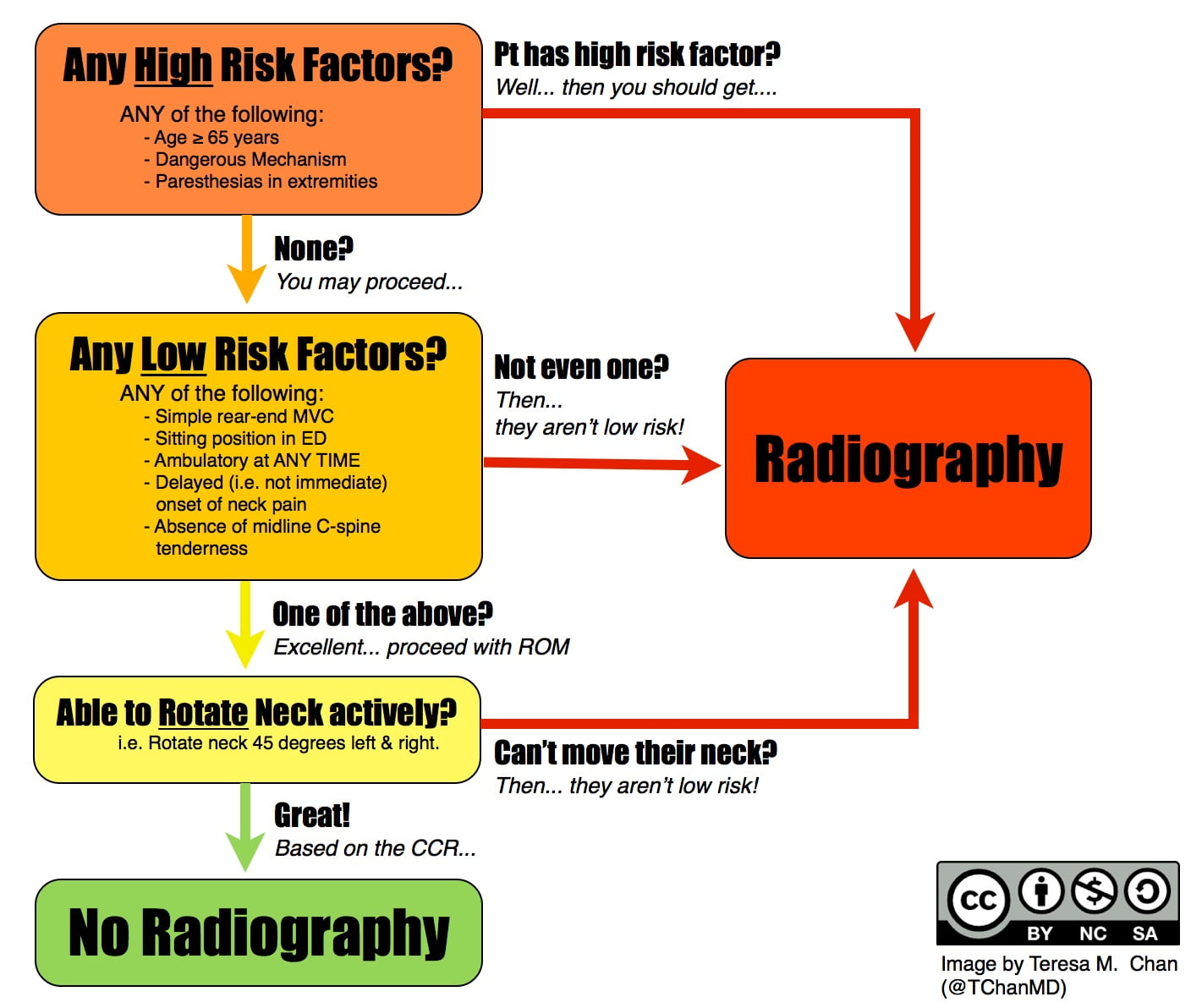 |
Table 1. Canadian C-Spine Rule Exclusion Criteria
Age < 16Minor injuries and not fulfilling inclusion criteria
Glasgow Coma Scale score <15
Grossly abnormal vital signs
Injury > 48h old
Penetrating trauma
Acute paralysis
Known vertebral disease (ankylosing spondilitis, rheumatoid arthritis, spinal stenosis, previous spinal surgery)
Return visit for reassessment of same injury
Pregnant
The NEXUS criteria was developed by Hoffman and colleagues in 1998 and is validated for use in the ED. It consists of five low-risk criteria; if the patient does not meet all five criteria, he or she requires C-spine x-rays. These criteria include: No posterior midline cervical spine tenderness; no evidence of intoxication; normal level of alertness; no focal neurologic deficit; and no painful distracting injuries. (See Figure 2) “Intoxication” and “level of alertness” are further defined in the original paper; these criteria and “painful distracting injury”, however, must be interpreted by the attending physician. The only exclusion criteria are patients with penetrating trauma and those who had a C-spine x-ray for reasons other than trauma. The NEXUS criteria are simple to use and can be widely applied to the ED patient population.
Figure 2. NEXUS Criteria (i.e. Table 2, from Hoffman et al. 1992)
1. No midline tenderness.
2. No focal neurologic deficits.
3. Normal alertness.
4. No intoxication.
5. No painful distracting injury.
The sensitivity of both rules for detecting clinically significant C-spine injuries in their own validation studies were 100%. A recent systematic review, however, found sensitivities for CCR and the NEXUS criteria of 90-100% and 83-100%, respectively. Furthermore, one study directly comparing the two rules showed better diagnostic accuracy for the CCR. Both rules, if applied appropriately, have the potential to reduce imaging rates (by 44% for CCR and 36% for NEXUS criteria).
As a final caution, although the NEXUS criteria have no age limitation, clinicians must beware of its use in the elderly. A recent study found a reduction in NEXUS criteria sensitivity from 84.2% to 65.9% in elderly patients (age ³65) with acute blunt trauma when compared to non-elderly patients. Physicians should have a low threshold for CT in this population.
Bottom line:
When compared to the NEXUS criteria, the CCR is slightly more complicated and has stricter exclusion criteria, but it has higher sensitivity.
Physicians should be aware of the populations to which these rules apply and can benefit from knowledge of both. Patients that may not be evaluated adequately with one tool can potentially be evaluated with the other. Both the NEXUS criteria and the CCR should be used as tools, not rules. And as always, clinical judgment and appropriate interpretation are key.
…. Back to the Case
Back to the case. Using CCR, the patient has no high-risk criteria, and she has at least one low risk criteria allowing assessment of active range of motion (ambulatory on scene, simple rear-end motor vehicle collision). When assessed, she can rotate her neck 45° right and left. She does not require imaging.
By NEXUS criteria, however, she requires imaging due to midline C-spine tenderness.
Challenge: Based on the above information – What would you do? Answer below!
[bg_faq_start]
Reviewing with the Staff | Dr. Rob Green (Click here to expand)
The use of appropriate radiologic investigation is important for patient diagnosis and management in the ED. Some evidence demonstrates that the use of radiologic investigations (especially CT scans) which may prolong patient time in the ED and increase exposure to radiation. Studies which limit radiologic investigations in low risk patients while “not missing” significant diagnosis are very important to our practice.
The CCR and NEXUS are 2 of these studies, both with positives and limitations outlined above – clinicians need to be aware of each study and utilize based on their patient and practice environment.
Thankfully, we have high quality studies to support limiting C-spine X-rays in low risk patients.
Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin)
Professor, Dalhousie University
Medical Director, Trauma Nova Scotia
Department of Critical Care Medicine
Department of Emergency Medicine
[bg_faq_end]
[bg_faq_start]References (click to expand)
Derivation NEXUS
Hoffman, J. R., Wolfson, A. B., Todd, K., & Mower, W. R. (1998). Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Annals of emergency medicine, 32(4), 461-469.
Validation NEXUS
Hoffman, J. R., Mower, W. R., Wolfson, A. B., Todd, K. H., & Zucker, M. I. (2000). Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. New England Journal of Medicine, 343(2), 94-99.
Derivation CCR
Stiell, I. G., Wells, G. A., Vandemheen, K. L., Clement, C. M., Lesiuk, H., De Maio, V. J., … & Worthington, J. (2001). The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA, 286(15), 1841-1848.
Validation CCR
Bandiera, G., Stiell, I. G., Wells, G. A., Clement, C., De Maio, V., Vandemheen, K. L., … & Worthington, J. (2003). The Canadian C-spine rule performs better than unstructured physician judgment. Annals of emergency medicine, 42(3), 395-402.
Coffey, F., Hewitt, S., Stiell, I., Howarth, N., Miller, P., Clement, C., … & Jabbar, A. (2011). Validation of the Canadian c-spine rule in the UK emergency department setting. Emergency Medicine Journal, 28(10), 873-876.
Vaillancourt, C., Stiell, I. G., Beaudoin, T., Maloney, J., Anton, A. R., Bradford, P., … & Wells, G. A. (2009). The out-of-hospital validation of the Canadian C-Spine Rule by paramedics. Annals of emergency medicine, 54(5), 663-671.
Stiell, I. G., Clement, C. M., O’Connor, A., Davies, B., Leclair, C., Sheehan, P., … & Wells, G. A. (2010). Multicentre prospective validation of use of the Canadian C-Spine Rule by triage nurses in the emergency department. Canadian Medical Association Journal, 182(11), 1173-1179.
Systematic review
Michaleff, Z. A., Maher, C. G., Verhagen, A. P., Rebbeck, T., & Lin, C. W. C. (2012). Accuracy of the Canadian C-spine rule and NEXUS to screen for clinically important cervical spine injury in patients following blunt trauma: a systematic review. Canadian Medical Association Journal, cmaj-120675.
NEXUS in the elderly
Goode, T., Young, A., Wilson, S. P., Katzen, J., Wolfe, L. G., & Duane, T. M. (2014). Evaluation of cervical spine fracture in the elderly: can we trust our physical examination? The American Surgeon, 80(2), 182-184.
[bg_faq_end]
Alana Hawley
Latest posts by Alana Hawley (see all)
- Medical Concept: Nicotine toxicity, a new trend in toxicology - August 31, 2015
- Boring Question: Which low risk C-spine rule is best? - September 11, 2014
Latest posts by BoringEM (see all)
- Pre-Game: CaRMS Interview Preparation - December 20, 2017
- Tiny Tips: SALTR for Pediatric Growth-plate Fractures - May 20, 2016
- Does that condition require investigation? - May 10, 2016