
All the content from the Blood & Clots series can be found here.
CanMEDS Roles addressed: Medical Expert, Health Advocate
Case Description
A patient is admitted to the internal medicine ward and after 5 days of clinical stability, she develops respiratory failure and is admitted to ICU. After 72 hours of mechanical ventilation her D-Dimer is increasing, and she develops worsening oxygenation. When should one suspect PE in COVID-19, and how to establish the diagnosis?
Main Text
PE diagnosis in COVID-19 patients is challenging. Many of the features of PE, such as shortness of breath and hypoxemia, are very common in patients with COVID-19, even in the absence of PE. Further, the diagnostic tests that we rely on, such as CT scans, may not be immediately accessible in a pandemic environment. While imaging should be obtained as soon as possible, it is important to not delay treatment in high risk cases. As a result, a presumptive diagnosis of PE may need to be made (and anticoagulation started) based on less information and certainty.
COVID-19 is a prothrombotic disorder
Any diagnostic approach for VTE should begin with consideration of how common clots are in the population of interest (i.e. pre-test probability). For hospitalized patients with COVID-19, we expect a higher rate of PE or DVT diagnosis than in non COVID-19 patients. Reports suggest that up to 40% of patients with severe COVID-19 infections may develop symptomatic blood clots despite being on prophylactic or intermediate dose (e.g. 50% dose) blood thinners1–3. Our patient’s risk for blood clots is further increased due to ICU admission 1.
Consider PE if sudden or unexplained cardiorespiratory decompensation or signs/ symptoms of DVT
The next step in the diagnostic evaluation is clinical assessment for features of PE and DVT. Unfortunately, clinical probability tools such as the Wells score have not been well tested in COVID-19 and many of the features they include are common in hospitalized patients making application troublesome. Given the high prevalence of blood clots in severe COVID-19 patients, we recommend considering PE for any patient with sudden or unexplained respiratory decompensation. A clinical assessment for features of DVT or other blood clots should also be done (unilateral extremity erythema, swelling or tenderness, dialysis, or ECMO clots). However, the majority of patients will ultimately not actually have a PE. For this reason, while we advocate for a high level of vigilance, further work up is required prior to confirming a PE diagnosis and starting treatment.
D-Dimer is insufficient to rule in or rule out PE
An elevated D-Dimer is a negative prognostic factor in the clinical course of COVID-19. However, the correlation between thrombosis and D-Dimers in these patients is less clear 4,5. For example, in an ICU study, despite a much higher rate of PE in the COVID-19 group, the D-Dimer elevations were actually higher in the general ICU population 2. As in the general population, D-Dimer can rise due to many different factors including renal failure, superimposed bacterial infection, or worsening COVID-19 infection 6. While, D-Dimer elevations are seen in sicker patients and sicker patients get more PE’s, an increased D-Dimer in patients with COVID-19 is not specific to an acute PE. Consequently we suggest the following:
- Elevated D-Dimers should not be used to rule in PE in patients with COVID-19, but sudden or unexplained elevations should raise suspicion.
- Low or stable D-Dimer values should not be used to rule out a PE in patients with COVID-19 if there is ongoing clinical suspicion for blood clots.
Standard of care imaging modalities (CT, U/S dopplers) should be used whenever possible if suspicion for PE
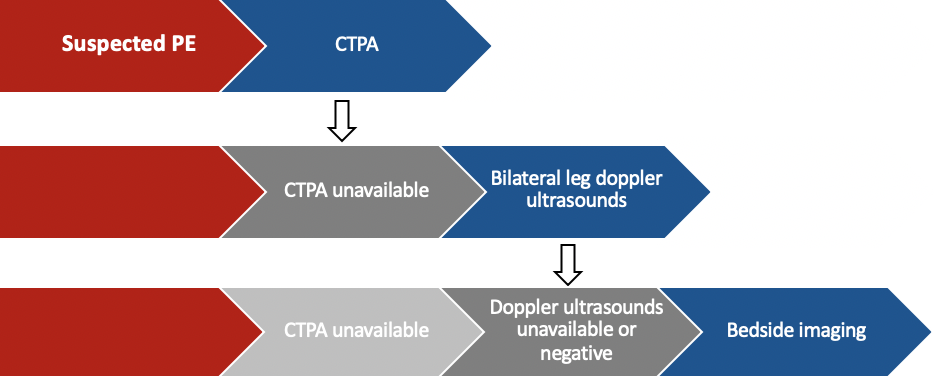
In keeping with guideline recommendations, patients with COVID-19 who have features concerning for PE should undergo standard of care diagnostic imaging (e.g. CTPA, doppler ultrasounds, etc.)7. In most cases, CTPA is the best option as it maintains accuracy in COVID-19 infection and has the added benefit of identifying alternative causes for the patients symptoms. Unfortunately, due to abnormal baseline CXR’s, VQ scans are often not useful in COVID-19 cases. If CT is not available, formal doppler ultrasounds should be obtained to assess for DVT. If a DVT is found, lung imaging can be deferred.
- CTPA is the first choice for most patients suspected of PE
- Standard of care doppler ultrasound (prioritized over bedside doppler ultrasound) for DVT can be considered if CTPA is not accessible
If diagnostic imaging is not available a presumptive PE diagnosis can be made on a case-by-case basis
If imaging is not accessible or there is suspicion for PE despite negative ultrasounds, a presumptive diagnosis can be established based on gestalt impression. Ancillary findings such as non-compressible veins on bedside ultrasound or right heart strain on bedside echocardiogram may suggest clots but these tests have relatively high rates of both false positives and false negatives.
In these cases, diagnosis of PE leads to a change in treatment so the question that needs to be addressed is whether there is enough evidence of PE to justify anticoagulation. This threshold is not static but dependent on the patient’s clinical status. For example, in a patient who is hemodynamically stable but has high risk of bleeding on anticoagulation, a greater emphasis is placed on definitively establishing a PE diagnosis. Conversely, in a patient who is clinically decompensating it may be reasonable to make a presumptive PE diagnosis based on less evidence. In all cases, a definitive diagnosis should be made at the earliest opportunity.
Case Conclusion
The patient develops respiratory failure after a period of clinical stability from their COVID-19 infection. Combined with a high baseline pre-test probability of PE (severe COVID-19 infection) this presentation is concerning for an acute PE. While D-Dimer elevation does occur in patients with PE, this is non-specific and a PE diagnosis cannot be made from a D-Dimer alone. A CTPA (or bilateral doppler ultrasounds if CT unavailable) should be obtained next. If no imaging is available, a presumptive PE diagnosis can be made (with imaging as soon as possible) as the patient is unstable and PE is felt to be the most likely cause. Bedside imaging that demonstrates right heart strain or a DVT supports a PE diagnosis but is not definitive.
Main Messages
- COVID-19 is a prothrombotic disorder and PE should be considered for sudden or unexplained respiratory changes.
- For most cases, no single clinical or laboratory feature (e.g. D-Dimer) is enough to rule in or rule out PE in COVID-19 by itself
- When PE is considered, diagnosis should be based on the standard of care imaging test (positive CTPA or doppler ultrasound) whenever possible. If imaging is not accessible a presumptive diagnosis can be made (and anticoagulation started) taking into consideration ancillary findings, clinical stability and bleeding risk.
All the content from the Blood & Clots series can be found here.
This post was reviewed by Brent Thoma, Nadia Omri and copyedited by Rebecca Dang.
- 1.Middeldorp S, Coppens M, Haaps TF, et al. Incidence of venous thromboembolism in hospitalized patients with COVID‐19. J Thromb Haemost. Published online July 27, 2020:1995-2002. doi:10.1111/jth.14888
- 2.Helms J, Tacquard C, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. Published online May 4, 2020:1089-1098. doi:10.1007/s00134-020-06062-x
- 3.Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thrombosis Research. Published online July 2020:145-147. doi:10.1016/j.thromres.2020.04.013
- 4.Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. Published online April 2020:844-847. doi:10.1111/jth.14768
- 5.Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. Published online April 27, 2020:1094-1099. doi:10.1111/jth.14817
- 6.Weitz JI, Fredenburgh JC, Eikelboom JW. A Test in Context: D-Dimer. Journal of the American College of Cardiology. Published online November 2017:2411-2420. doi:10.1016/j.jacc.2017.09.024
- 7.Spyropoulos AC, Levy JH, Ageno W, et al. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID‐19. J Thromb Haemost. Published online August 2020:1859-1865. doi:10.1111/jth.14929

Zachary Liederman