

Welcome back to our second post on the Ontario Emergency Department (ED) Return Visit Quality Program (RVQP). In our first post we discussed the utility of return ED visits as triggers for potential quality improvement (QI) initiatives. We also discussed the scope of this program, which is a provincial-level program with many stakeholder organizations. The program was built with the goal of promoting “high-quality ED care by helping clinicians and hospitals identify, audit and investigate underlying causes of return visits to their ED and take steps to address these causes, preventing future return visits and harm”.1
The RVQP is a great example of continuous QI methodology that leverages health information technology (HIT). The program would not be possible without this HIT infrastructure due to its provincial scope, number of interacting stakeholders, sheer number of data elements, data security requirements, and timelines. The continuous flow of information from patient registration in the ED to audits being performed necessitates an organized set of standards for data collection, storage, transfer and integration.

It is important for stakeholders to appreciate the inner workings of the RVQP, just as a driver of a car should know some basics of what is “under the hood”. There are several reasons why some knowledge of the HIT background of the RVQP may be helpful to front-line clinicians:
- It provides key insights into the architecture of the program they are involved in.
- It provides a model for provincial-level QI programs.
- It engages clinicians as key stakeholders in the program.
- It provides clinicians with an illustrative paradigm for information technology in the healthcare setting.
Informing clinicians on the HIT inner workings of the RVQP empowers them to be more active participants in not only contributing to the program’s success, but also in providing feedback to further improve it. This is a key element in classical QI methodologies. For example, with lean methodology, front-line staff are empowered to identify problems as they arise so that they can be immediately addressed.
If we wanted to describe the RVQP’s architecture from a health informatics perspective, we may want to do so with an organized approach. There are a multitude of frameworks that can be used for this purpose; however, we found using the Informatics Stack framework to be the most applicable and comprehensive.2 Similarly structured approaches are utilized in understanding a process in QI methodology, for example with root cause analyses driver diagrams or fish bone diagrams. These frameworks help us understand a process or system in a comprehensive manner to allow further synthesis.
The Informatics Stack
The Informatics Stack is a conceptual framework that seeks to describe the architecture of HIT programs through a series of hierarchical levels from most comprehensive to most basic. Figure 1. illustrates its various levels and their descriptions.3
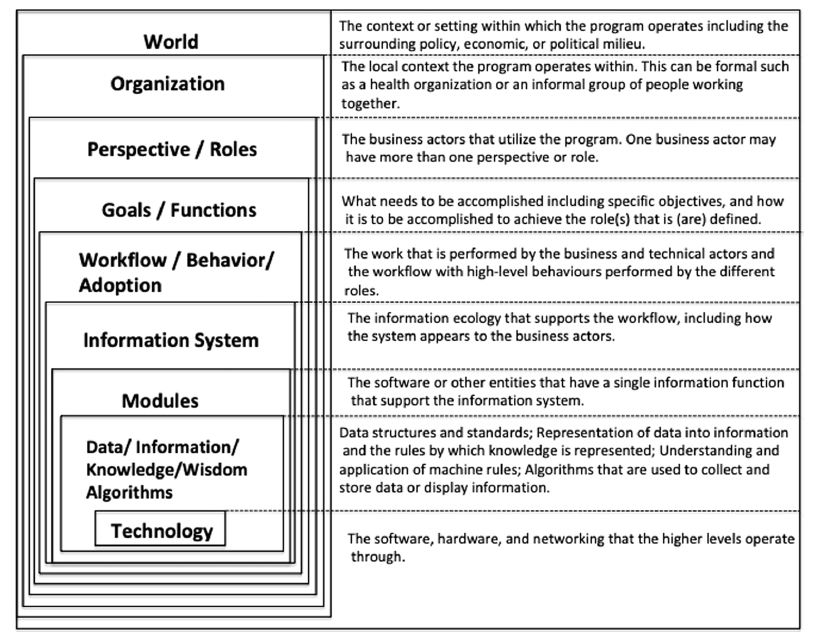
Adapted from Lehmann H. 2017 2
The Informatics Stack is used to provide a description of a HIT program at each level. It provides a comprehensive description of the architecture of the RVQP to enable a thorough understanding and potential for replication. A full description of the RVQP across the informatics stack levels was published in 2019.3 For our discussion of the RVQP here, we will highlight two levels to illustrate the program scope and workflow. These are the organizational level and the workflow level. We will also discuss some of the enablers of the RVQP from an informatics perspective.
The Informatics Stack: Organization Level
The ED RVQP spans 86 EDs and five main stakeholder organizations. Each organization has its specific mandate and its contributions to the program. Any changes to one organization’s contributions may have an effect on the other organizations and the program itself. There is both top-down and bottom-up communication with a Ministry of Health mandate and participating EDs, with national and provincial organizations in the middle. Their description and roles are described in Table 1.
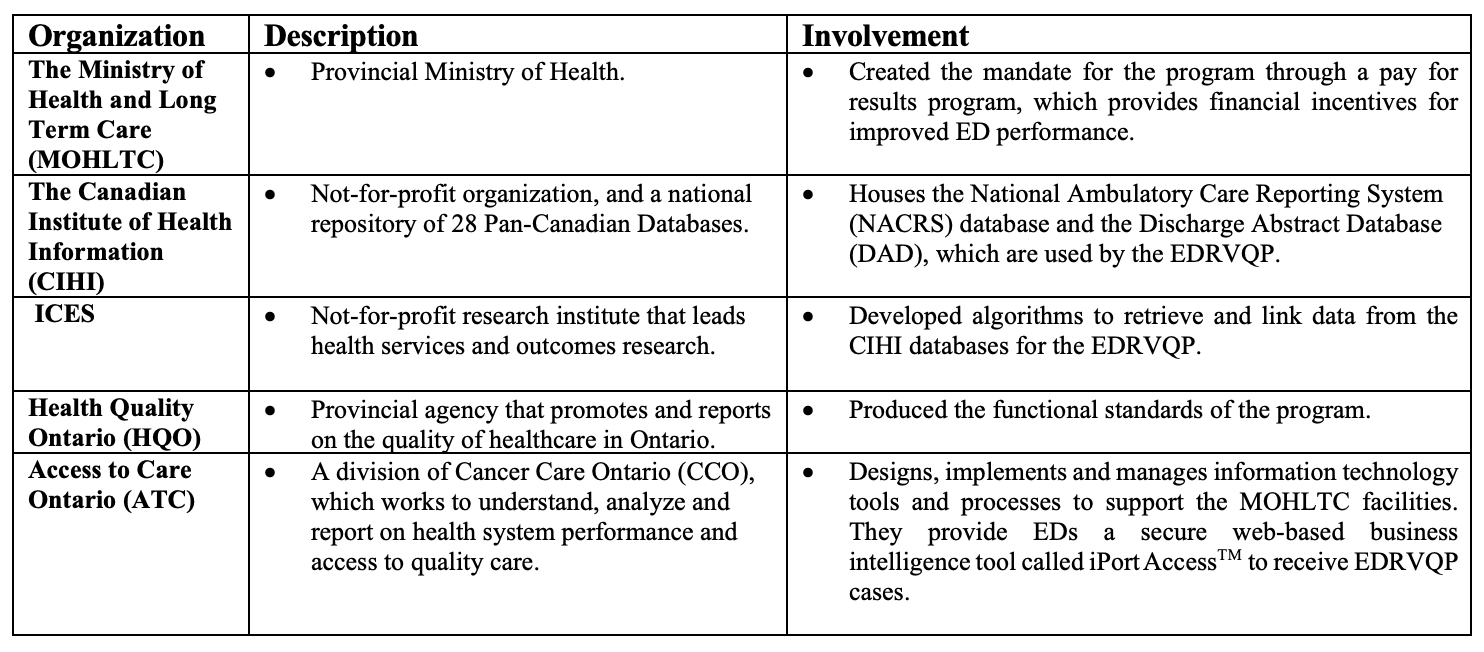
*Adapted from Taher et al.3
The Informatics Stack: Workflow / Behaviour / Adoption Level
As an ED physician, you see a patient and discharge them home. You are notified six months later that a return visit occurred and may need further analysis. But what happens in the middle? Data flows from the ED and hospital ward discharges, and is then integrated via predefined algorithms. This data is then shared back with the EDs, which then audit the returns based on pre-specified auditing guidelines. Figure 2 illustrates the overall health informatics architecture of the program:
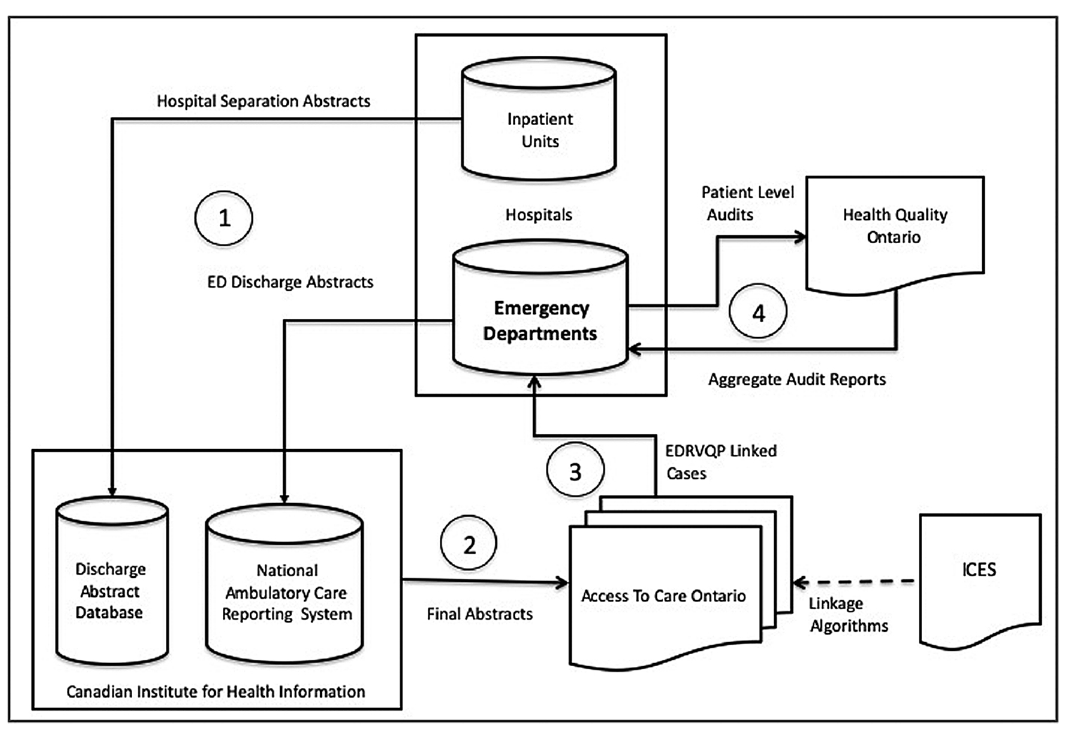
Adapted from Taher et al.3
Enablers and Barriers
The success of a provincial-wide continuous QI program is contingent upon certain enabling factors. The attributes of success of a program of this scope include both a legislative mandate (top-down) and implementation flexibility (bottom-up) with stakeholder-driven contributions. There is a reliance on both technology adoption and standardized use (functional standards). Moreover, leveraging and seeking support from other EDs to assist in program implementation is arguably one of the most important aspects of the RVQP in creating a provincial QI culture. A survey of stakeholders identified the key enablers illustrated in Table 2 as being crucial to the success of the program.3

Adapted from Taher et al.
EHR – Electronic Health Record; HQO- Health Quality Ontario; CIHI- Canadian Institute for Health Information; ICD-10 CA International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada; CCI – Canadian Classification of Health Interventions; HL7 – Health Level 7
Quality Improvement and Health Informatics
The ED RVQP is a great example of applying continuous QI methodology that leverages health information technology. Through the use of validated algorithms and functional data standards, the program overcomes many barriers of manual data collection and analysis at the provincial level. Moreover, it provides security, and scalability to the program if it were to expand to other provinces. With increasing uptake of new information technologies, new opportunities will arise to improve regional continuous quality improvement programs. It is important for clinicians to have some background on the inner workings of the program to optimize participation, empower solutions, and sustain a culture of QI in the ED.
That’s it for this post, join us next time where we discuss some of the great accomplishments of the RVQP and lessons learned.
Thank you to Lisa Fuller, Emily Hayes, and Ivan Yuen from Ontario Health (formerly Health Quality Ontario) for their input.
Senior Editor: Lucas Chartier
Junior Editor: Ed Mason
**UPDATE (November 2020): The HiQuiPs Team is looking for your feedback! Please take 1 minute to answer these three questions – we appreciate the support!**
- 1.Health Quality Ontario. Introductory Guidance – the ED Return Visit Quality Program. Health Quality Ontario.; 2017.
- 2.Lehmann H. The Informatics Stack: A Heuristic Tool for Informatics Teaching. Methods Inf Med. January 2017:e129-e133. doi:10.3414/me16-01-0152
- 3.Taher A, Bunker E, Chartier LB, et al. Application of the Informatics Stack framework to describe a population-level emergency department return visit continuous quality improvement program. International Journal of Medical Informatics. January 2020:103937. doi:10.1016/j.ijmedinf.2019.07.016

Ahmed Taher
Latest posts by Ahmed Taher (see all)
- HiQuiPs: Managing Crises – What’s going on behind the scenes? - June 4, 2024
- HiQuiPs: Root Cause Analysis in the Time of COVID-19 - May 14, 2024
- Expert’s Corner – Dr. Eddy Lang on Quality Improvement and Healthcare - July 29, 2021

Howard Ovens