
All the content from the Blood & Clots series can be found here.
CanMEDS Roles addressed: Medical Expert
Case Description
A pregnant 32 year old female presents to the ER with chest pain. She is 33 weeks gestational age, and this is her third pregnancy (two prior uneventful deliveries). Her pain started 3 hours ago while she was watching television. It is sharp, worse with inspiration, and located along the right costal margin. She has mild dyspnea at rest. She denies any palpitations or hemoptysis, and has no complaints of calf or thigh discomfort. She is otherwise healthy with no prior history of venous thromboembolism (VTE), and takes only a prenatal vitamin.
On exam her heart rate is 102, blood pressure 115/70, oxygen saturation 96% on room air, and respiratory rate is 22. Her weight is 80 kg. Cardiac and respiratory examinations are unremarkable. She has no leg swelling or erythema. Her abdomen demonstrates a gravid uterus.
Her bloodwork demonstrates a Hb of 98, WBC 5.0, platelets 156, creatinine 80. D-Dimer is 1,080. Her chest x-ray is unremarkable, with no effusions or consolidation.
Does she have a pulmonary embolism (PE)?
Main Text
Question 1: How helpful are clinical prediction rules and D-Dimer for ruling in or ruling out pulmonary embolism in pregnancy?
The problem with diagnosing pulmonary embolism in pregnancy is that dyspnea and tachycardia are very common during normal pregnancy, particularly in the third trimester. It’s true that the risk of VTE is higher during pregnancy by 5 to 10 times (with the highest risk in the postpartum period). However, given the low baseline risk of VTE in young women overall (1 in 10,000), the absolute risk of VTE in pregnancy is still not very high. For example, in Canadian the incidence of PE is 5.4 cases per 10,000 pregnancies 1.
Unfortunately, our usual clinical prediction rules (such as the Wells Score for PE) are not applicable to pregnant females because the studies that derived these scores excluded them. The specificity of the Wells criteria is questionable in pregnancy as tachycardia and leg edema are common in normal pregnancy. The ability to assess an “alternative diagnosis” is also difficult in pregnancy 2.For these reasons, most obstetrical guidelines suggest against the use of clinical prediction rules to rule out VTE (including PE).
What about the D-Dimer? Same issue. A D-Dimer, which is typically used to rule out VTE in the setting of a low clinical pretest probability, has not been validated in the pregnant population. Pregnant women were generally excluded from the studies which established the use of D-Dimer in the diagnosis of PE. Given the aforementioned issues in establishing a pretest probability, it is unclear how to interpret the D-Dimer in pregnancy. The D-Dimer in normal pregnancy typically increases with gestational age, and the threshold of a “positive” D-Dimer is not known. While smaller observational studies have proposed that alternative D-Dimer thresholds may be applicable in pregnant patients, these thresholds have not been evaluated in prospective management studies that examine their utility in combination with pregnancy-specific clinical prediction rules. As such, the D-Dimer’s utility in pregnancy for excluding PE is uncertain and has not been sufficiently validated in this group of patients 3.
Question 2: Which diagnostic test should be ordered to evaluate for suspected pulmonary embolism in pregnancy?
Given the above limitations, objective imaging is needed to exclude PE. Our choice of test should take into account the need for a definitive diagnosis, while minimizing the potential for harm to both the developing fetus and to the mother (breast tissue and future carcinogenesis). The radiation dose required for either V/Q scanning or CT-PA is below the teratogenic fetal dose of radiation, and should not be a contraindication to performing definitive imaging if required.
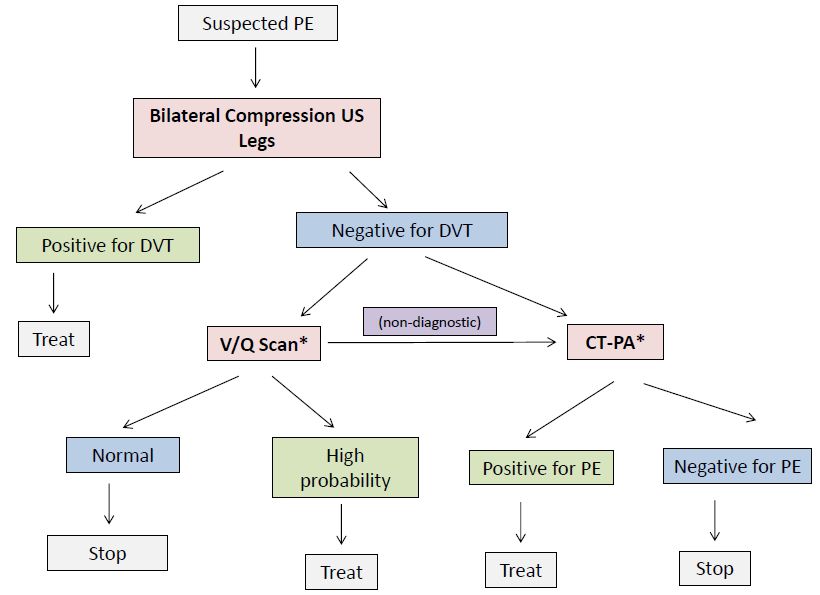
The strengths and weaknesses of four choices are outlined below in Table 1. A possible diagnostic algorithm for pulmonary embolism in pregnancy can also be found in Figure 1.
Table 1: Imaging options for exclusion of PE in pregnant women
| Test | Strengths | Limitations |
| Bilateral leg compression ultrasound (US) |
|
|
| Chest x-ray (CXR) |
|
|
| CT pulmonary angiography (CT-PA) |
|
|
| Ventilation / Perfusion Scan (V/Q) |
|
|
Guidelines from multiple societies vary 5, 6, 7, 8 in their recommendations about whether a CT-PA or V/Q scan is preferred as the definitive imaging test. Ultimately, your choice will depend on what is available at the time your patient presents, and the local radiology (CT-PA) or nuclear medicine (V/Q scan) expertise.
One reasonable approach that is commonly employed is similar to the principles outlined by the European Society of Cardiology from 2014 5, which states:
- Perfusion scintigraphy (ie. V/Q scan) may be considered to rule out suspected PE in pregnant women with normal CXR (Class IIB recommendation)
- CTPA should be considered if the CXR is abnormal or if lung scintigraphy is not readily available (Class IIa recommendation)
Given the variability in guidelines and equipoise about the preferred front-line imaging test to rule out PE, I generally discuss the benefits and risks of V/Q scanning versus CT-PA with my patient when deciding which test to pursue. Here is one possible approach that incorporates the possibility of using either test (* denotes equipose):
Case Conclusion
You send your patient for bilateral leg ultrasounds, which do not demonstrate evidence of DVT. The nuclear medicine department is unable to complete a V/Q scan at night and your patient expresses concerns about the risks of radiation to breast tissue, so you give her one empiric dose of anticoagulation (Dalteparin 15,000 units) and arrange for a V/Q scan in the morning.
The V/Q scan is high probability for pulmonary embolism, with a perfusion defect present in the right upper and middle segmental arteries. You start her on Dalteparin 15,000 units SC daily and arrange for follow-up with Thrombosis Clinic the next morning (see next blog post!).
Main Messages
- Clinical prediction rules such as the Wells Score are not valid for pregnant individuals and should not be used in this setting
- D-Dimer testing in pregnant patients has not been prospectively validated in management studies to exclude VTE, and as such its utility is uncertain in this group of patients
- V/Q scan or CT-PA are safe in pregnancy for mom and baby, and the choice of first diagnostic imaging test should be made after engaging in shared decision making with patients after discussing the advantages and drawbacks of each modality
All the content from the Blood & Clots series can be found here.
This post was reviewed by Jesse Leontowicz, Brent Thoma, and copyedited by Rebecca Dang.
References
Eric Tseng
Latest posts by Eric Tseng (see all)
- Blood & Clots Series: Subsegmental PE – To Treat or Not To Treat? - June 25, 2020
- Blood & Clots Series: Is Fecal Occult Blood Testing helpful in deciding whether it’s safe to prescribe anticoagulants? - April 30, 2019
- Blood & Clots Series: How do I manage acute VTE in pregnancy? - September 25, 2018