

Why is this topic important?
As a learner, you will inevitably experience “difficult” encounters during patient care. In fact, clerks and junior residents are more likely to label patient encounters as “difficult”.1 These encounters often involve patients that refuse to answer questions, use profanity, demand specific investigations or treatments, and express frustration with wait times. But why is it important for clerks and junior residents to learn how to handle difficult encounters with patients? One of the most important reasons is providing quality healthcare for all patient populations.
What makes an encounter difficult?
The reasons for difficulties during patient encounters can be grouped into three categories: the learner, the patient, and the environment1.
The Learner – The emergency department (ED) is fast-paced. While clerks are not expected to work as quickly as residents or staff physicians, we still feel pressure to work efficiently and perform at our best. This pressure drives a fierce desire for us to succeed in each interview, causing clerks to become invested in our suggested diagnostic or management plan for the patient. Accordingly, we can become frustrated when we receive constructive feedback, which is particularly common with these difficult encounters . Aside from performance anxiety, we may be more susceptible to ascribing bias to our patients before we even meet them. For example, a quick look through a patient’s chart can reveal a large list of prior ED visits for vague or unresolved complaints, altering our perception of the patient. These personal factors can predispose us to failure in difficult interactions, irrespective of the patient or environment.
The Patient – Perhaps the most frequent frustration in the ED is caused by long wait times, but patient’s frustration may be caused by many other factors, including a fear of their current illness. For patients with chronic illness, frequent visits to the ED may be a reminder of the daily burden of living with their illness. Frequent ED visits driven by social circumstances, like homelessness or substance use, may be viewed similarly. Recurrent ED visits caused by these circumstances also increase the odds of having a poor clinical encounter because each visit can turn into a difficult encounter. Beyond illness, frequent visits, and wait times, other factors like language and cultural barriers may leave patients feeling misunderstood or disrespected. These are but a few causes for patient frustration in the ED. Just remember: A) the patient likely has a legitimate reason for their frustration, and B) your job is to determine the source of the patient’s frustration to appropriately address the underlying cause.
The Environment – Every aspect of the ED is optimized to improve workflow, wait times, and patient outcomes. However, patients may not see this, and may wait unknown periods of time to be triaged, roomed, and treated. Often, patients only spend a few minutes with each healthcare provider, repeating their story multiple times. In this system, patients are relegated to a dependent role and have no control over their care. Added to the lack of control is the depersonalization these patients experience. It is easy to feel like just another sick person in an ED system that values efficiency over comfort. It is no surprise this environment can frustrate patients.
How can I diffuse the tension during a difficult encounter?
There is no one size fits all method for dealing with difficult encounters. The approach below reflects a combination of techniques from several sources to create an approach for dealing with difficult encounters2.
Set Up the Problem – The first phase of dealing with a difficult encounter can be broken into three parts:
- Identify that this is a difficult interaction
- Gain emotional control
- Start with a good first impression
The first part of any difficult encounter is recognizing that there is a problem. This part of the interaction is crucial and is often missed by junior learners. You may notice your patient is frustrated before you meet them by talking with their nursing staff. Similarly, a quick look through their medical records can signal any previous difficulties. Should you encounter a tough patient, internally acknowledge it is a difficult encounter and start addressing it immediately.
Once you identify a difficult interaction, take a moment to gain emotional control to target the “self” factor discussed above. Engaging a patient by arguing may be a natural response in a normal conversation, but is guaranteed to make a physician-patient interaction worse. In this scenario you can benefit from reframing a difficult interaction. Instead of viewing a difficult encounter as a barrier to impressing your preceptor, approach the interaction as an opportunity to showcase your communication skills and independence in dealing with a tough situation.
Finally, begin every interview with a good first impression. Starting with a proper introduction, eye contact, and a smile reassures the patient that you are there to help them. Walking into a room with crossed arms and a stressed or frustrated demeanor will not.
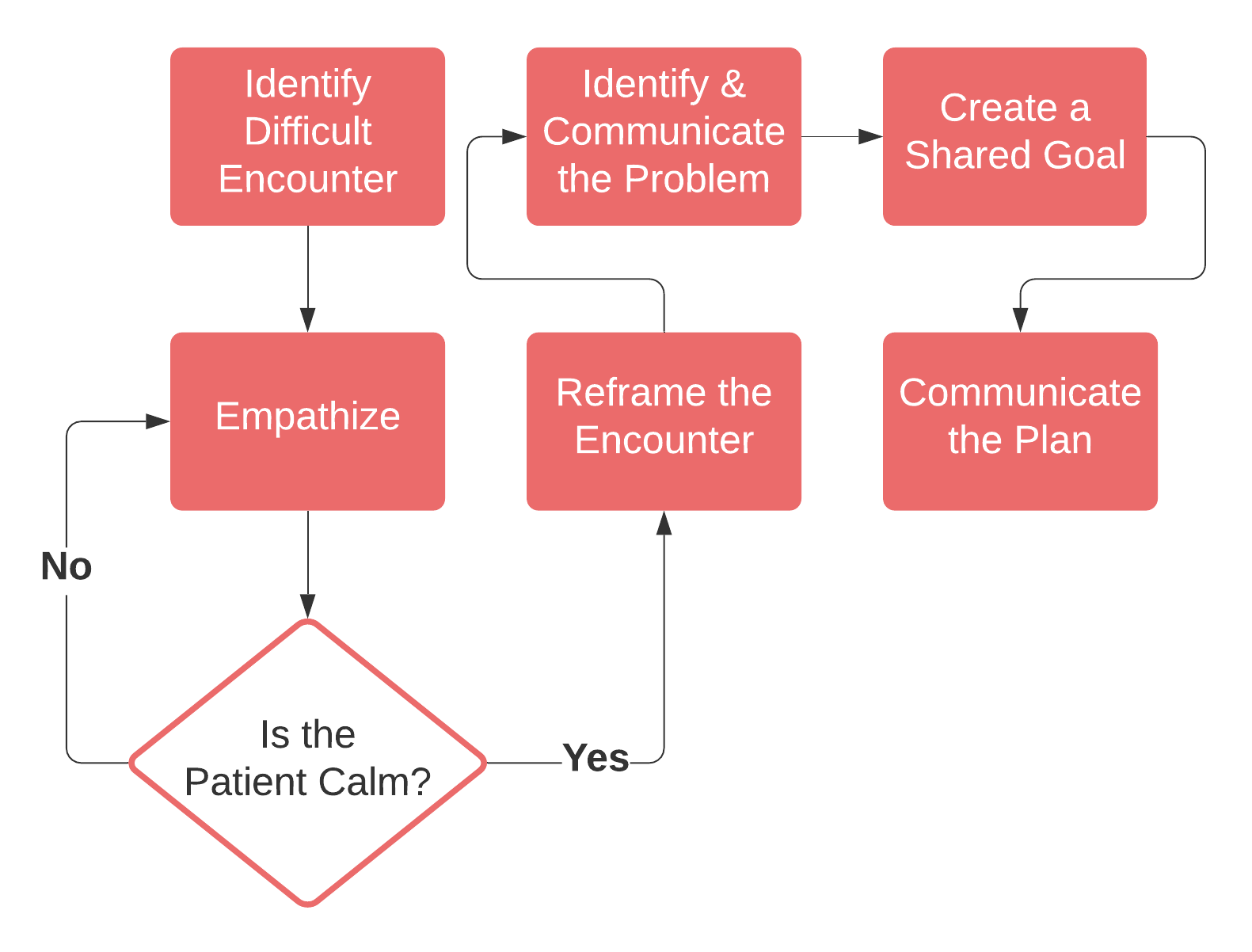
Help them Calm Down – The next step in any difficult interaction is to calm the patient. There are a variety of tips and tricks you can use including:
- Empathize
- The Broken Record
- Use Silence
- Leave the Room
- Get Help
The best technique for calming patients is to empathize. Assure the patient that your role is to listen to their concerns and validate their emotions. Phrases like, “I’m here to listen,” and, “You seem upset, I want to understand why so I can help address your concerns,” reinforce your role as a listener. Validating statements such as, “I would also be upset if I were in your shoes,” and “I understand why you’re upset” let the patient know that you are on their side. Most patients will calm down within minutes once they have been given time to express their frustration.
If the patient does not calm down, Dr. Walter Himmel suggests a series of four excellent strategies. One of the easiest tricks is the Broken Record technique. Repeat what the patient says to express you are listening and on the patient’s side until they begin to calm. This is effectively continuing to empathize until the patient cools off.
Using silence may also calm a confrontational patient. Providing a moment of silence allows the patient to logically consider their emotions, de-escalating the situation.
If the patient remains upset, consider leaving the room so that they can cool off. Sometimes the best strategy is allowing the patient to contemplate their anger alone. This strategy is also effective if you find you are becoming frustrated as well. It is better to avoid engaging in an argument that could permanently damage your relationship with the patient. It is critical that you leave the room if you question your safety at any point. For more information on dealing with physically threatening patients, CRACKCast episode 187 “The Combative and Difficult Patient,” is an excellent resource.
Solve the Problem – Once the patient is calm, you may then address the problem and create a plan. This part of the approach targets the “patient” and “environment” factors by discovering the cause of the problem and giving the patient control in the encounter. No matter if your patient is swearing at you, demanding a CT scan, or refusing treatments, the following steps will defuse the situation:
- Reframe the Encounter
- Determine Why the Patient is Upset
- Communicate the Problem
- Create a Shared Goal
The first part of solving the problem is to demonstrate that you and the patient are on the same team. This is where reframing comes in. Reframing changes the encounter from an argument to a conversation by aligning your shared goals with the patient’s. Statements such as, “It’s okay to be upset, I want to understand more so I can help us fix the problem” can help reframe the interaction. Reframing will help win the patient over and determine the underlying source of their frustration.
If the patient did not tell you why they were frustrated when you were calming them down, you have to ask directly. Try saying, “You seem [anxious / upset / concerned], can you tell me why?”.
Once you identify the origin of the problem, communicate it. This ensures you are correct and reiterates to the patient that you are on the same page. Next, ask for their cooperation with a statement such as “I need you to help me by [answering a few questions / sitting down / etc.]”. This engages the patient by creating a shared goal and gives them a sense of control.
At the end of the interview, you must communicate a clear plan with your patient. Let them know you will return to discuss the plan in a few minutes when you have reviewed your findings with your preceptor. Communicating a plan is helpful in many difficult encounters2.
[bg_faq_start]Example Case
It’s 7 pm and you’ve just aced a presentation on your patient with chest pain. Two patients into your shift and you’re confidently settling into the rhythm of another busy shift in the ED. Your preceptor sends you to see a new patient, Darren, a 52 year old man with a four day history of lower back pain. After introducing yourself Darren replies “Finally, I’ve been laying here in pain waiting to see someone for hours.” You offer a brief apology and continue on with the history which seems like a slam dunk for mechanical lower back pain. As you feel the history coming to a close Darren says, “The reason I came today is to get an MRI so I can figure out what’s going on, and I’m not leaving until I get one”.
Practice using the approach to difficult encounters algorithm to navigate this interaction
Using the Approach
| Setting up the problem | By greeting you with a hostile response, Darren demonstrated this interaction could be difficult. At this point mentally preparing for a difficult interaction will ensure you aren’t taken off guard by an aggressive comment later on. Preparing early reduces the chance you react with anger. |
| Empathize / Identify the problem | Directly address Darren’s frustration with a phrase like, “I get the feeling you’re upset, can you tell me why?” This allows you to determine the root of his problem and empathize to calm him down. |
| Reframe the Encounter | Let Darren know you also want to figure out the cause of his back pain. An example might sound like, “I also want to try to learn what’s causing this pain. I’m going to do my best to get you an answer.” |
| Address the problem | While we don’t know the underlying problem for certain in this example, part of it is definitely linked to Darren’s perception of MRI’s utility for his condition. Addressing the low likelihood of relevant MRI findings and risks like increased risk of unnecessary intervention for incidental findings could be helpful. |
| Create a Mutual Goal / Communicate the Plan | Ask Darren for his cooperation with a thorough physical exam. Explain the importance of an exam in determining the cause of his pain. Communicate that abnormal exam findings may necessitate additional imaging, and a normal exam rules out the need to image. While performing the exam explaining what you are testing can demonstrate you are being thorough in exploring a variety of potential causes for his back pain. |
Common Encounters that can Place You in a Difficult Situation
Being Drawn into Conflict
As junior learners we worry about our performance and are inexperienced when it comes to difficult encounters, increasing our tendency to respond with confrontation.
How you can avoid it:
- Avoid seeking a perfect outcome from the encounter, by investing less emotion in the outcome, you can respond objectively.
- If you feel yourself becoming frustrated, Dr. Himmel in EM Cases episode 52 suggests taking a second to mentally recite, “I’m alert, I’m alive, and I feel good”.
Explaining the Triage System
When patients are upset because of long wait times it feels natural to explain there were other patients with urgent medical problems who needed to be seen first. However, all a frustrated patient hears is that they waited longer because they were less sick.
How you can avoid it
- This is the perfect opening for reframing. When a patient expresses frustration with wait times, apologize. Then assure them you want to provide efficient (and thorough) care so you can send them on their way.
Failing to Set Boundaries
We often allow patients to continue behaving inappropriately to avoid confrontation. Establishing boundaries controls the situation and improves the odds of having a successful interaction.
How you can avoid it:
- Be firm but not too firm. Reframe the situation by calmly asking the patient to change their behavior.
- Recognize you have little to lose. If setting boundaries fails, the patient continues to act inappropriately and you have not lost any real ground. If they respond positively you are one step closer to a successful interaction.
Summary
In difficult encounters with patients there are plenty of reasons for why the interaction can go wrong, including factors relating the learner, the patient, and the environment. Break difficult interactions into three main steps: setting up the problem, calming the patient, and solving the problem. To set up the problem identify that it is a difficult interaction, gain emotional control, and start with a good first impression. Calming the patient starts with empathizing. If empathizing is unsuccessful try techniques including the broken record, silence, leaving the room, and calling for help. Finish the interaction by communicating the problem and setting a mutual goal with the patient. Junior learners, residents and staff physicians alike will encounter difficult interactions. Learning how to manage these situations early in your training will set you up for success throughout your career.
This post was edited and uploaded by Megan Chu.
[bg_faq_start]Resources
This episode of Emergency Medicine Cases provides an excellent discussion on how to deal with difficult encounters, including tips and tricks for executing many of the topics discussed in this post.
For a deep dive, the journal article “The General Approach to the Difficult Patient” contains a discussion on factors that contribute to difficult interactions. It also includes a comprehensive approach to difficult interactions based on commonly encountered scenarios (note: this article is not open access).
For an approach to violent or physically aggressive patients, CRACKCast episode 187 provides an excellent summary of the Rosen’s Emergency Medicine textbook chapter on The Combative and Difficult Patient.
The Canadian Medical Protective Association also has a statement on “Difficult patient encounters: What you can do to prevent, manage, and de-escalate.”
[bg_faq_end]References
- 1.Hahn SR, Kroenke K, Spitzer RL, et al. The difficult patient. J Gen Intern Med. Published online January 1996:1-8. doi:10.1007/bf02603477
- 2.Allespach H, Marcus EN, Bosire KM. Sailing on the ‘7 Cs’: teaching junior doctors how to redirect patients during difficult consultations in primary care. Education for Primary Care. Published online April 10, 2017:46-48. doi:10.1080/14739879.2017.1312554
Reviewing with the Staff #1
Though the medical literature is riddled with the term “difficult patient”, I personally feel that this is a really patronizing term and would challenge all trainees to think about this as an antiquated term like “pimping” (which Dr. Eve Purdy, has previously ranted about). I think this piece takes a really good perspective on how we can rethink the paradigm of including ourselves in the situation and acknowledge our role in creating high tension scenarios.


Reviewing with the Staff #2
This is an excellent topic to review for both the medical trainee and staff physician. Difficult encounters can present challenging scenarios where knee-jerk reactions can result in escalating conflict, or worse, medico-legal action. Having a set of go-to verbal techniques, such as expressing empathy and intentionally using a slow and calm voice, can be crucial in these situations. Furthermore, I have found that these patients are often hungry or cold, and offering to meet these basic needs can help demonstrate that you are working together rather than in opposition.
As a staff physician, I like to be involved whenever there is a difficult physician-patient encounter. During my general orientation with learners, I will use the common phrase of, “If there is any patient who is medically unstable or you’re worried about, let me know right away” to which I also add, “If there is any patient who you’ve had a difficult interaction with or who states they are dissatisfied with their care, let me know right away as well.” I feel that becoming involved as the staff physician gives the patient a chance to re-express their concerns as well as the medical team the chance to explain the treatment plan, which ideally opens up an opportunity for reconciliation.


Alexander Wyma