

The Case
You’re in the final stretch in an overnight fast track shift at your local emergency department andsleepily contemplating whether to invest in another energy drink when you glance over at the triage desk and your natural endorphins kick in.
A 25-year-old male with the presenting complaint of left shoulder pain is being seen – and the dude has obvious pathology.

(Not actual file photo – this image shows similar patient with pathology on opposite arm – From Imagine courtesy: http://thesportsphysio.wordpress.com/2013/08/20/shoulder-instability-part-2-trauma/)
You immediately suspect an anterior shoulder dislocation and gleefully attempt a Cunningham reduction while taking your history. The patient notes a one-week history of increasing left shoulder instability. His past medical history is significant for previous dislocations of both shoulders. He is otherwise well and takes no medications. He awoke with the shoulder discomfort and came in straight away.
Unfortunately, your reduction is not successful and you start thinking about that energy drink again. You slink off to order a series of shoulder films.
Play along! For the following images (actual file photos), name the view and note the presence of any abnormalities. Discussion below.

What is this view? Any abnormalities?

What’s this view? What bony anatomy comprises the important landmarks?

What’s this view called? How do we know which direction is anterior and which is posterior?
Acute Posterior Dislocations of the Shoulder
This patient presents with an acute posterior shoulder dislocation.
General Information & Incidence
Posterior shoulder dislocations are rare, accounting for only 2-4% of all shoulder dislocations (anterior dislocations make up the vast majority). The shoulder support provided by the scapulae and their thick muscular associations is what makes this type of dislocation so uncommon. Posterior shoulder dislocations are generally associated with the ‘3 Es’: ethanol, epilepsy, and electricity. The mechanism of injury is nearly always indirect traumatic force, such as a fall or seizure.
Delays in the diagnosis of posterior shoulder dislocation are common due to subtle clinical and radiographic findings. ED physicians must be vigilant and look for them.
Clinical Assessment & Presentation
This patient presented classically, with an internally-rotated arm held in adduction, with reluctance and pain on external rotation.
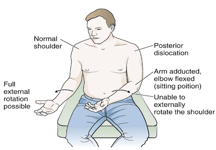
Image courtesy Roberts & Hedges Clinical Procedures in Emergency Medicine (6th ed) 2014. Philadelphia. Elsevier Saunders Inc. – Chapter 49
Other findings in posterior dislocation may include:
- Anterior contour of the shoulder absent (flattened anterior shoulder),
- Prominent coracoid and acromion,
- Rounded posterior shoulder,
- Palpable posterior humeral head
Radiographic Examination
In the setting of a suspected posterior shoulder dislocation, radiographs should be surveyed for several subtle findings. In particular, a full shoulder series (anterior-posterior (AP), scapular ‘Y’, and axillary views) is an essential part of the diagnostic workup. Occasionally, a patient’s inability to externally rotate for the ordered views (as noted by the radiology tech) may be a helpful clue in the case of a unsuspected posterior dislocation.
AP View
Subtle signs on the AP radiograph include:
- ‘Light Bulb sign’
- Internally rotated humeral head appears symmetric on AP film (due to rotation of the greater tuberosity).
- ‘Empty glenoid sign’
- Widened space between articular surface of humeral head and anterior glenoid rim.
- Trough sign
- Dense vertical line on AP indicating compression fracture of medial aspect of humeral head.
| Abnormal Image A | Normal AP View | Un-Boring Finding |
|---|---|---|
 |  |  |
| Empty glenoid fossa and widened joint space | Humeral head well-positioned and overlaps with glenoid fossa | 'Lightbulb Sign' due to rotation of greater tuberosity of humeral head; 'Trough Sign' on humeral head |
Scapular View
The scapular view is generated by superimposing the humeral head over the coracoid, acromion, and scapular body and spine. A posterior dislocation is represented by the humeral head lying posterior to the glenoid fossa.
| Abnormal Image B | Normal Scapular 'Y' View | Un-Boring Finding |
|---|---|---|
 |  |  |
| Humeral head appears misleadingly well-positioned in this view - this is why multiple views are essential! | Humeral head overlying intersection point of coracoid, acromion, and scapular spine | Posterior dislocation of humeral head (HH - humeral head; G - glenoid, SP - scapula) |
Axillary View
| Abnormal Image C | Normal Axillary View | Un-Boring Finding |
|---|---|---|
 |  |  |
| Posteriorly displaced humeral head with reverse Hill-Sachs lesion | Humeral head well-positioned in relation to the glenoid fossa | Coracoid process points anteriorly; note posterior displacement of humeral head; arrow shows reverse Hill-Sachs lesion |
The axillary view is generated by placing the arm in abduction, with the image taken through the axilla at 45 degrees. This is arguably the most important view for posterior dislocations, as it easily visualizes a posteriorly situated humeral head. It may also reveal the presence of a reverse Hill-Sachs lesion (also known as a McLaughlin defect), which is an impaction fracture of the humeral head following posterior dislocation.
Tip: Use the coracoid process to orient yourself to the anterior direction on the film!
Reduction Technique

From Roberts & Hedges Clinical Procedures in Emergency Medicine (6th ed) – Chapter 49
As with any dislocation, be sure to check neurovascular status prior to reduction! Fortunately, neurovascular injury is rare in posterior dislocation because the nerves and vessels serving the area are protected due to their anterior location. Consider ortho involvement as posterior dislocations are rare and they may want to be involved in the reduction. Reverse Hill-Sachs lesions occur in >20-25% of posterior dislocations and may require open reduction and internal fixation (ORIF) under general anaesthestic, which is another good reason to consult orthopaedic surgery. Patients in whom you suspect a reverse Hill-Sachs lesion may require further imaging (CT) prior to reduction.
To reduce a posterior dislocation, apply traction to the internally-rotated and adducted arm in conjunction with direct pressure on the posterior aspect of humeral head. The mechanics are relatively similar to the traction-countertraction technique sometimes used to reduce an anterior dislocation.
Analgesia
Consider procedural sedation with or without an intraarticular block for adequate muscle relaxation and patient anxiolysis.
Post-reduction care
Repeat neurovascular examination and post-reduction radiographs are key. On assess of shoulder ROM the patient should now be able to place palm of injured arm on the opposite shoulder. The patient will require post-sedation monitoring, shoulder immobilization, and follow-up with ortho.
Case Resolution
After your refreshing energy drink, you review the case with your attending. You note the presence of a subtle empty glenoid sign on AP film, and posteriorly displaced humeral head with a reverse Hill-Sachs lesion on axillary view. You suspect a posterior shoulder dislocation.
After further discussion with the patient, he confides that he is worried that he may have seized prior to presentation because when he awoke with the shoulder pain he felt groggy and his bedding and bedside items were on the floor. Apparently he’s had a few of these before with unremarkable neurology workups.
The shoulder reduced without issue and the patient is referred to neurology for further workup of for his possibly recurrent seizures.
Peer reviewed by Dr. Sarah Luckett-Gatopoulos (@SLuckettG) and staff reviewed by Dr. Heather Murray (@HeatherM211)
References
- Roberts & Hedges Clinical Procedures in Emergency Medicine (6th ed) 2014. Philadelphia. Elsevier Saunders Inc. – Chapter 49
- Tintinalli’s Emergency Medicine: A Comprehensive Study Guide (7th ed) 2011. New York. McGraw Hill Companies Inc. – Chapter 268
- Rosen’s Emergency Medicine: Concepts and Clinical Practice (8th ed) 2014. Philadelphia. Elsevier Saunders Inc. – Chapter 53
More Posterior dislocations on FOAMed..
- Life in the Fast Lane – Posterior Shoulder dislocation (Great images of the radiographic signs mentioned above)
- The Blunt Dissection – ‘In or Out?’
- EM Resident Blog – Case Discussion
- Radiopaiedia – Posterior Shoulder Dislocations
Corey Veldman
Latest posts by Corey Veldman (see all)
- Posterior Shoulder Dislocation: Radiographic Evidence - October 6, 2014
Latest posts by BoringEM (see all)
- Pre-Game: CaRMS Interview Preparation - December 20, 2017
- Tiny Tips: SALTR for Pediatric Growth-plate Fractures - May 20, 2016
- Does that condition require investigation? - May 10, 2016