
Frostbite occurs when tissues are exposed below their freezing point of -0.53oC for a period of time1. We think of frostbite occurring in winter, but it’s important to remember that serious injuries can occur secondary to refrigerant chemicals, dry ice, CO2 fire extinguishers, expanding propane, or other similar products. Outside of occupational injuries, some of the strongest risk factors for developing frostbite are homelessness, psychiatric illness, alcohol consumption, and inadequate or ill-fitting clothing.1,2 Unfortunately, many of these risk factors are seen together in emergency department patients. Since the initial presentation of freezing injuries can be subtle and appear deceptively benign, patients are at risk of being overlooked in a busy department. It’s important to recognize these injuries in vulnerable people and provide rapid care to improve outcomes.
Much like strokes and heart attacks, in frostbite, some cells are killed while many others are only injured and have the potential to be salvaged with optimal care. So, although the injury has already occurred, our actions can significantly impact patient outcomes. As an important reminder, we must treat life-threatening conditions, such as moderate to severe hypothermia, prior to turning our attention to frostbite.
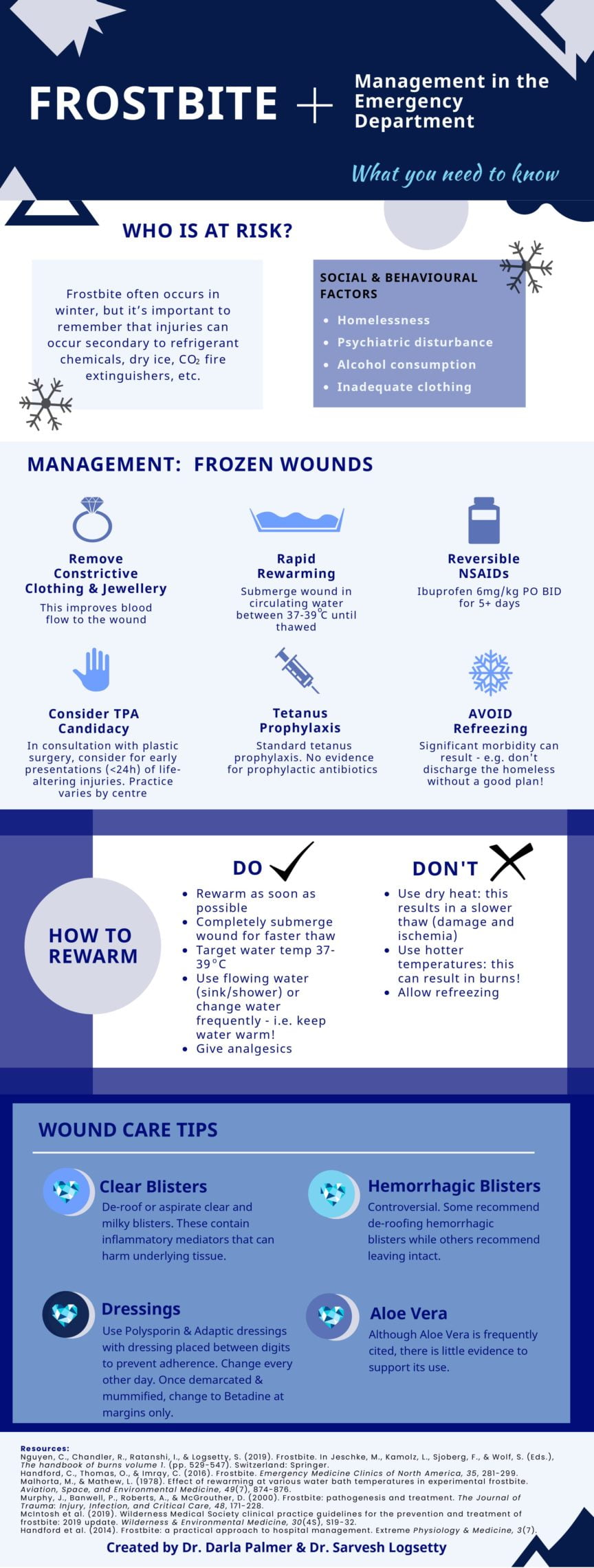
Treatment recommendations:
- Remove constrictive clothing and jewelry
- Constrictive items should be removed to improve blood flow to the wound. Once these restrictions are removed, the area often swells. If the patient is still in the field this may be problematic as boots or gloves may not be able to be replaced once removed.2
- Rapid rewarming
- The wound should be rewarmed as soon as possible.
- Rewarmed by submerging in water between 37 to 39oC until the skin becomes soft, pliable,1,3–5 and remains warm. If available, use whirlpool to keep the water consistently warm; otherwise, use a shower or sink with flowing water.
- Do not use dry heat, such as heaters or fires. Air is a poor conductor of thermal energy resulting in a slower thaw. It is also harder to control the temperature using these methods which may result in burns1,5.
- Active motion should be encouraged, but the skin should not be massaged as this may result in mechanical trauma and does not improve blood flow.2 The tissues should also not touch the sides of the tub which may result in mechanical injury.5
- Rewarming is intensely painful and will require analgesia.
- Never allow a wound to re-freeze. If a thawed tissue may refreeze, it’s safer to delay treatment.5
- NSAIDs
- NSAIDs block the production of prostaglandins and thromboxane, which are responsible for the vascular stasis and late ischemic phases of injury
- Initiate a minimum dose of 12mg/kg divided twice daily of ibuprofen starting as soon as possible.1,5 The dose can then be increased further for its analgesic effects. If ibuprofen is not an option, aspirin can be used.5 Recommendations for duration of therapy is variable. Please refer to your local practice guidelines.
- The evidence for this is limited, but there is minimal relative risk from a short course of NSAIDS.
- Thrombolytics
- The use of thrombolytics remains highly controversial. If used they should be initiated within 24 hours of injury and for a potentially life-altering injury, such as bilateral thumbs or a limb. Please refer to your local practice guidelines and consult your local plastic surgery team.
- Iloprost
- Iloprost is a synthetic prostaglandin analogue that inhibits platelet aggregation, contains vasodilatory properties, and may contribute to fibrinolysis.1,5,6 The evidence to support its use is limited and it is not approved for use in Canada.
- Wound care
- Except as needed for the rewarming, the limb should be elevated since this will help prevent edema formation. Edema is thought to worsen progressive dermal ischemia and puts the tissue at higher risk for infection.6
- Deroof or aspirate clear and milky blisters. The fluid in blisters contain prostaglandins and thromboxanes which are thought to cause further damage to underlying tissue.6
- Hemorrhagic blisters suggest deeper injury to the dermal vascular plexus5. There is little evidence for hemorrhagic blister management and treatment remains controversial. Some feel that debridement may result in desiccation which could be more harmful to underlying tissues while others feel that the blood in the blisters acts as a potential media for infection.6
- Aloe vera is thought to inhibit local thromboxane formation, however, there are few human studies to support its use.
- Prophylactic treatments
- Standard tetanus prophylaxis should be given to the patient.5,6
- There is no evidence to support the use of prophylactic antibiotic therapy.5,6
- Dressings
- Topical antimicrobial dressings similar to that used for burn injuries should be started (e.g. double antibiotic ointment and a nonadherent petrolatum fine mesh gauze). Once demarcated and mummified the dressings can be simplified to painting the margin between viable and nonviable tissue with betadine and dressing open.
- Surgery
- Early surgery is not recommended and may result in unnecessary morbidity as it is very difficult to predict tissue loss. Amputations should be delayed for one to three months once clear demarcation occurs.5
This post was copyedited by Casey Jones (@CaseyMAJones). A PDF version of the infographic can be downloaded here.
References
- 1.Nguyen C, Chandler R, Rantanshi I, Logsetti S. Frostbite. In: Jeschke M, Kamolz L, Sjoberg F, Wolf S, eds. The Handbook of Burns Volume 1. Vol 1. Springer; 2019:529-547.
- 2.Handford C, Thomas O, Imray C. Frostbite. Emerg Med Clin North Am. 2017;35(2):281-299. doi:10.1016/j.emc.2016.12.006
- 3.Malhotra M, Mathew L. Effect of rewarming at various water bath temperatures in experimental frostbite. Aviat Space Environ Med. 1978;49(7):874-876. https://www.ncbi.nlm.nih.gov/pubmed/666681
- 4.Murphy J, Banwell P, Roberts A, McGrouther D. Frostbite: pathogenesis and treatment. J Trauma. 2000;48(1):171-178. doi:10.1097/00005373-200001000-00036
- 5.McIntosh S, Freer L, Grissom C, et al. Wilderness Medical Society Clinical Practice Guidelines for the Prevention and Treatment of Frostbite: 2019 Update. Wilderness Environ Med. 2019;30(4S):S19-S32. doi:10.1016/j.wem.2019.05.002
- 6.Handford C, Buxton P, Russell K, et al. Frostbite: a practical approach to hospital management. Extrem Physiol Med. 2014;3:7. doi:10.1186/2046-7648-3-7
Reviewing with Staff
Frostbite often results in injury, with significant life altering effects. Amputations can range from tips of digits to whole hands and limbs. Survivors of frostbite often have lifelong pain and challenges in caring for themselves. Unfortunately populations who are already resource challenged are at increased risk for frostbite. Few single centres have significant numbers of frostbite to garner extensive experience. Therefore, there are no large studies to guide practice. As a result there is a wide variability in the management of frostbite. These guidelines provide an initial framework for the care of the patient with acute frostbite, and will hopefully help to reduce the dramatic consequences. The mainstay is rapid moist rewarming which should be done as soon as possible. Adjuncts such as tPA and Iloprost should be discussed with your local referral centre once rapid rewarming has been completed. The addition of an anti platelet agent (NSAID) is relatively low risk with significant potential benefit, especially when used for a short course (3-5 days). We encourage all readers who treat frostbite to contact the Canadian Frostbite collaborative, or the American Burn Association Frostbite advisory group for future information.
Logsetty Biography:
Dr. Sarvesh Logsetty is a Professor of surgery with cross appointments in psychiatry and pediatrics. His interest is the longterm effects of burns and traumatic injury. He is a member of the Canadian Frostbite Collaborative, and the American Burn Association Advisory Group for Clinical Practice Guidelines on Frostbite. He has over 80 book chapters and peer reviewed publications. His current research endeavours are focused on creating a new burn dressing, and better understanding the social determinants of health as they apply to injury and injury prevention.


Darla Palmer
Latest posts by Darla Palmer (see all)
- Emergency Management of Frostbite - January 11, 2022
Sarvesh Logsetty
Latest posts by Sarvesh Logsetty (see all)
- Emergency Management of Frostbite - January 11, 2022