
You are working on a busy overnight shift in your local emergency department. You are comfortable with your flow, but feel that you are subject to some inefficiencies including finding the next patient’s chart, and different paper order sets, and having to write out lengthy discussions that you had with patients. You are often forced to put on your detective hat as you try to decipher previous handwritten notes in your patient’s chart. Your hospital is moving towards implementing a new electronic health record (EHR) system in the coming year and you are curious about whether the new health record system will solve your inefficiencies.
Welcome to another HiQuiPs post. In our previous Health Informatics posts we discussed an introduction to biomedical health informatics, as well as Computerized order entry and patient safety. For this post, we take a step back and discuss the basics of EHR systems as preparation for their use in the ED context. You may wonder why this is important for clinicians? ED clinicians learn the basics of many tools they use including casting material, the slit lamp, suturing material and their stethoscope. Learning the basics of EHR systems empowers clinicians to better use these tools and their many functionalities, to have better discussions with their information technology specialists about optimization or troubleshooting, and to building solutions that better fit their clinical context and workflow.
Electronic Health Records
People refer to electronic health, patient or medical records as well as personal healthcare records. Several of these terms appear to be used interchangeably but have some small differences as illustrated by the Canada Infoway definitions 1
Electronic Medical Record : A partial health record under the custodianship of the healthcare provider(s), which holds a portion of the relevant health information about a person over their lifetime. Often used within the bounds of the organization. For example, the system that is present in a general practitioner’s office.
Electronic Health Record: A complete health record under the custodianship of healthcare provider(s) that holds all relevant health information about a person over their lifetime. This can be used across organizations in a longitudinal manner. For example, a hospital electronic health record system that can share and receive information with other systems and organizations.
Personal Health Record: A complete or partial health record under the custodianship of a person(s) (e.g. a patient or family member) that holds all or a portion of the relevant health information about that person over their lifetime. For example, current consumer products include apple health or google fit profiles.
For a clinician’s everyday use, usually we refer to EHRs, EMRs or electronic patient records (EPRs) interchangeably to denote an electronic system to document and gather information about patients. Moreover, when used today in the clinical realm we are often referring to the EHR system that contains active tools to manage the information and integrate with other electronic tools used in patient care to facilitate information sharing and decision making.
EHR System functional components
When clinicians think of EHRs they mainly think of the documentation. However there are five basic functional components of an EHR system:2
Integrated view of patient data
Patient data is found across various forms including text, images, videos, lab and radiology information system findings, administrative data, etc. Each form of data can have its own form of storage and standards related to its use (more on this in a future post!). This allows the integration of multiple sources of data with potential ease of access, privacy oversight and efficiency. If you do use an EHR system, think about what you can access with a couple of clicks.
Clinician order entry
A function that allows clinicians to make decisions and enter orders. This function forgoes errors from misreading hand writing. It can also use evidence-based orders, i.e. logic built into orders or order sets, time stamps, data collection on physician care practices, and integrated billing functions. An illustration of this was discussed in our previous post on computerized order entry and adverse drug reactions.
Clinical decision support
These functions go hand-in-hand with the clinician order entry. Decision support aids in the decision making and safe provision of care. This support harnesses the power of computing and increasingly, the presence of artificial intelligence (AI). From dosage calculations, reminders, alerts and built in algorithms. The EHR system can be infused with evidence based diagnostic and treatment approaches that assist clinicians in decision making.
Access to knowledge resources
This is a capability to retrieve more information on clinical questions that arise. Often these can be linked through commercial vendors such as electronic textbooks, UptoDate, MicroMedex, etc.
Integrated communication and reporting support
Given the increasingly complex and multidisciplinary interactions of clinicians across the patient care continuum, timely communication is an integral component. EHR systems can allow for clearly delineated reporting of the different clinical care teams across a patient’s care continuum. Functions may also exist to support direct communication between different clinicians through the EHR system, or even patients.
The EHR system as you will notice is a comprehensive system that allows for integration of information, knowledge generation, and decision making. Figure 1. illustrates a schematic of some of these basic functions. The user is depicted on the right of the figure interacting with the system on the left through the user interface (vertical line).
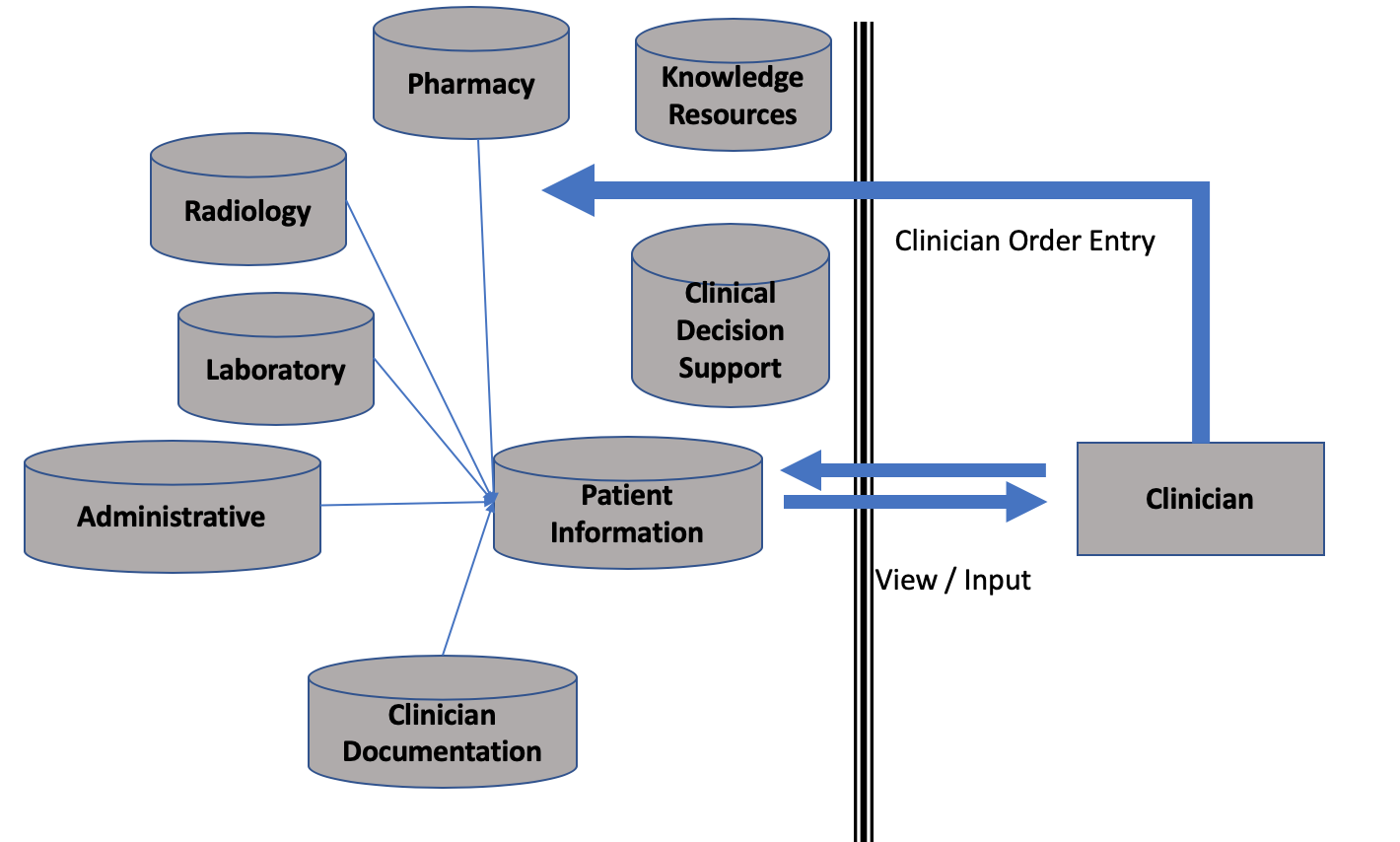
Figure 1. Electronic Health Record System Basic Functions
Best of Breed vs Monolithic Systems
Over the years, EHR systems have evolved beyond their basic functions. For example, EHR systems are now collecting data through wearable technology 3, and giving patients access to their own health records 4. There are also new systems for specific specialties such as pathology-specific database, and intensive care unit modules for critical care continuous patient monitoring etc. With increasing functionalities EHR system users find two basic setups in their organizations.2
Monolithic Systems
This is a single large system that contains all functions that are used by the organization such as in figure 1. These systems usually come with standard functions and design from the vendor and may allow some personalization depending on the clinical needs and workflow. Data sharing across applications is usually simplified as it is housed under one system with shared functional standards. However the specialized functions are limited by the amount of personalization that is allowed.
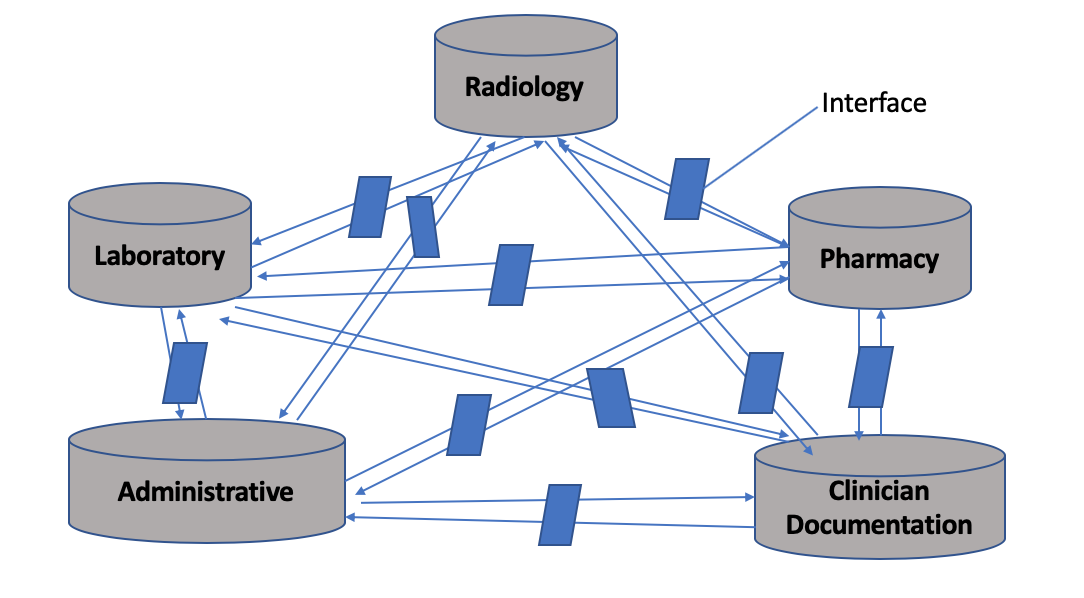
Best of Breed Systems
These are systems that are built with highly specialized functionality for each clinical context. Organizations would typically have to purchase different systems for each of their needs. This approach would allow better specialization for each clinical context but typically can run into challenges with information flow, needing the development of interfaces (ways to communicate and share data) between each of their systems. Imagine that each system needs a different interface with every other system that is present as Illustrated in figure 2. This becomes an exponential challenge when large organizations have 10s to 100s of different interfaces.
Summary
EHR systems have basic functions that allow clinicians to document, retrieve information enter orders and make decisions. Systems differ in complexity and in structure. EHR systems can be seen as a tool that is used as part of a clinician’s workflow. An understanding of the tool can empower clinicians to better use it and better engage with their information technology specialists to optimize it for their clinical domain.
Join us next time where we delve deeper into a discussion of system interoperability and the challenges it poses for clinicians.
Senior Editor: Shawn Mondoux
Junior Editor: Mark Hewitt
Copyedited by: Mark Hewitt
- 1.Hodge T. EMR, EHR, and PHR – Why All the Confusion? https://www.infoway-inforoute.ca/. https://www.infoway-inforoute.ca/en/what-we-do/blog/digital-health-records/6852-emr-ehr-and-phr-why-all-the-confusion. Published April 2011. Accessed March 27, 2020.
- 2.Shortliffe EH, Cimino JJ, eds. Biomedical Informatics. Springer London; 2014. doi:10.1007/978-1-4471-4474-8
- 3.Al-Azwani I, Aziz H. Integration of Wearable Technologies into Patients’ Electronic Medical Records . Quality in Primary Care. 2016;24(4):151-155.
- 4.Archer N, Fevrier-Thomas U, Lokker C, McKibbon K, Straus S. Personal health records: a scoping review. J Am Med Inform Assoc. 2011;18(4):515-522. doi:10.1136/amiajnl-2011-000105

Seyon Sathiaseelan
Latest posts by Seyon Sathiaseelan (see all)

Justin Majnarich
Latest posts by Justin Majnarich (see all)

Ahmed Taher
Latest posts by Ahmed Taher (see all)
- HiQuiPs: Managing Crises – What’s going on behind the scenes? - June 4, 2024
- HiQuiPs: Root Cause Analysis in the Time of COVID-19 - May 14, 2024
- Expert’s Corner – Dr. Eddy Lang on Quality Improvement and Healthcare - July 29, 2021