

This updated episode of CRACKCast covers Rosen’s Chapter 020, Sore Throat (9th Ed.). Sore throat is an extremely common ED presentation, that while can feel dry, is important to have a solid approach to due to uncommon, but severe infectious and airway sequelae.
Shownotes – PDF Here
[bg_faq_start]Rosen’s in Perspective
We can hear all of the sighs being bellowed out by all of our listeners in podcast-land. But, this complaint is often one of Dillan’s favourite triage note lines to read. Patients presenting with sore throat to the ED often times need little more than reassurance and NSAIDs. However, some can harbour serious pathology that require the clinician to acutely stabilize, investigate, and consult specialty services to get the patient the care they require. To get your blood pumping, let’s jump into today’s episode with a case:
You are working the afternoon shift at a community ED. You have been inundated with a multitude of CTAS 4’s and 5’s when you pick up the next chart. The patient, placed in the streaming area of the department, has a note that reads “Sore Throat – CTAS 5 – pain x 48 hours, patient seen 24 hours ago and diagnosed with strep throat. Patient appears ++ anxious.”” Triage vitals show the patient is febrile, mildly tachycardic (109 BPM), and tachypneic (RR 25).
You go back and hear the patient before you see them. You turn the corner, and the patient is tripoding, drooling, and stridorous.
What will you do? What are your next steps? How do you find a new pair of pants given that your current pair have been soiled?
Do not despair, listeners. We will be giving you all the tools you need to stabilize this patient. Additionally, we will give you the baseline knowledge you need to investigate the vast majority of patients presenting with sore throat. We will review the anatomy of the area in question, discuss the utility of imaging and antibiotics in the patient with sore throat, and will throw some quick snappers at you to put away for your next on-shift quizzing by the otolaryngologist on-call.
[bg_faq_end]Core Questions:
[bg_faq_start][1] What are the three anatomically-distinct zones of the pharynx, and what structures outline their borders?
- Nasopharynx
- Encompasses the area superior to the oral cavity
- Area lies between the base of the skull and the soft palate
- Eustachian tubes open into the nasopharynx
- Oropharynx
- Area directly behind the oral cavity between the uvula and hyoid bone
- Includes the epiglottis and vallecula
- Bordered laterally by the tonsillar pillars
- Hypopharynx
- Located inferior to the epiglottis
- Stops at the point at which the aerodigestive tract differentiates into the esophagus and larynx
- Inferior border is vocal cords
- External landmark = look just superior to the thyroid cartilage
[2] Describe the utility of the following imaging modalities in the patient with sore throat.
Ultrasound of Neck:
- Becoming increasingly useful to detect neck masses, tumors, and hypopharyngeal conditions
- Some studies indicate it has a role in the diagnosis of epiglottitis in males and females
- Not a mainstay in the work up of these pathologies, but stay tuned
Lateral Neck Radiography:
- Not a requirement to diagnose these conditions, but can be useful
- The lateral neck radiograph is
very sensitive for pathology related to retropharyngeal abscesses. Look for:
- Widening of the prevertebral space
- Abnormal curve of the C-spine
- Presence of soft tissue air
Nasopharyngoscopy:
- Can be useful at the bedside
- Primarily used to interrogate the pharynx in cases where the physical examination is not necessarily telling (e.g., profound sore throat, no obvious pathology on physical examination).
- Allows for the identification of:
- Infection
- Foreign bodies
- Polyps
- Angioedema
CT Soft Tissues Neck:
- Very useful imaging modality for serious soft tissue infections of the pharynx
- Definitive evaluation for deep space neck infections
- Consider in children or adults with signs and symptoms of deep space neck infections (e.g., retropharyngeal abscess) and in patients who may need airway management
- Sometimes difficult for CT to delineate between cellulitis and abscess
- Also helpful when trying to differentiate between tumors, hemorrhage, abscesses
[3] Outline five viral, five bacterial, and five other potential etiologies of sore throat in the ED patient? [Table 20.1]
The list below outlines the differential diagnosis for the patient with sore throat. It is adapted from Table 20.1 – Differential Diagnosis for Sore Throat in Rosen’s 9th Edition. Please refer to this table for further detail.
Viral Causes of Sore Throat:
- Rhinovirus
- Adenovirus
- Peptostreptococcus spp.
- Coronavirus
- HSV- 1,2
- Influenza A,B
- Parainfluenza
- Cytomegalovirus
- EBV
- VZV
- Hepatitis Virus
Bacterial Causes of Sore Throat:
Common Aerobic Causes:
- Streptococcus pyogenes
- GABHS
- Coccidioides spp.
- Non-GAS
- Neisseria gonorrhoeae
- Neisseria meningitidis
- Mycoplasma pneumoniae
- Arcanobacterium haemolyticum
- Chlamydia trachomatis
- Staphylococcus aureus
Uncommon Aerobic Causes:
- Haemophilus influenzae
- Haemophilus parainfluenzae
- Corynebacterium diphtheriae
- Streptococcus pneumoniae
- Yersinia enterocolitica
- Treponema pallidum
- Francisella tularenis
- Legionella pneumophila
- Mycobacterium spp.
Anaerobic Causes:
- Bacteroides spp.
- Peptococcus spp.
- Clostridium spp.
- Fusobacterium spp.
- Prevotella spp.
Systemic Causes of Sore Throat:
- Kawasaki Disease
- Steven Johnson Syndrome
- Cyclic Neutropenia
- Thyroiditis
- Connective tissue disease
Fungal Causes of Sore Throat:
- Candida spp.
Traumatic/Miscellaneous Causes of Sore Throat:
- Penetrating Injury
- Angioneurotic Edema
- Retained Foreign Body
- Anomalous Aortic Arch
- Laryngeal Fracture
- Calcific Retropharyngeal Tendinitis
- Retropharyngeal Hematoma
- Caustic Exposure
Neoplastic Causes if Sore Throat:
- Tongue cancer
- Larynx cancer
- Thyroid cancer
- Leukemia
[4] Outline the components of the Modified Centor Score and describe its application.
The Modified Centor Score helps to approximate the probability that pharyngitis is caused by Streptococcus pyogenes. Its elements are listed below:
Components of the Centor Score:
- Age
- +1 = 3-14 years
- 0 = 15-44 years
- -1 = >/ 45 years
- Exudate or
Swelling on Tonsils
- +1 = presence
- 0 = absence
- Tender/Swollen
Anterior Cervical Lymph Nodes
- +1 = presence
- 0 = absence
- Temperature
> 38.0 degrees Celsius
- +1 = presence
- 0 = absence
- Cough
- +1 = absence
- 0 = presence
Probability of Streptococcal Pharyngitis:
- Score 4/5 = 51-53%
- Score 3 = 28-35%
- Score 2 = 11-17%
- Score +1 = 5-10%
- Score -1 to 0 = 1-2.5%
Actions Based on Scores:
- Score 4/5 = perform rapid strep testing and/or culture – consider empiric antibiotics depending on clinical scenario – IDSA does not recommend empiric antibiotics in developed countries
- Score 3 = perform rapid strep testing and/or culture
- Score 2 = optional rapid strep testing and/or culture
- Score -1 to +1= No further testing or antibiotics
[5] Describe the diagnostic algorithm for the patient with sore throat. [Figure 20.4]
The following diagnostic algorithm is taken from Figure 20.4 Rosen’s Emergency Medicine, 9th Edition. Please refer to this figure for further details. In the patient presenting to the ED with sore throat:
- Determine
presence of upper airway compromise:
- Stridor
- Drooling
- Muffled voice
- Sniffing position
- Hypoxia
- If there are
signs of upper airway compromise:
- Look for
visual mass (e.g., PTA, tongue elevation, angioedema)
- If present, provide disease-focused therapies and consult ENT, Anesthesiology for airway surgical support
- If not, consult ENT for nasopharyngosocopy
- Consider one of the imaging modalities mentioned previously
- Look for
visual mass (e.g., PTA, tongue elevation, angioedema)
- If there are
no signs of airway compromise:
- Examine the
oropharynx to determine presence of pharyngitis
- If present, consider symptomatic treatment, consider antibiotics in high likelihood GABHS in endemic or epidemic settings of rheumatic fever
- If not present, consider non-pharyngitis causes of sore throat
- Examine the
oropharynx to determine presence of pharyngitis
[6] Outline the approach to managing a patient with sore throat in the ED. [Figure 20.4]
The following diagnostic algorithm is taken from Figure 20.4 in Rosen’s Emergency Medicine, 9th Edition. Please refer to this figure for further details.
In the patient presenting to the ED with sore throat:
- Determine
presence of upper airway compromise
- If present,
do the following:
- Prepare for potential surgical management
- Maintain an upright position
- Insert large-bore IV’s, place on cardiac monitors
- Consider empirical steroids, antibiotics
- Consider surgical service and Anesthesiology consultations for bedside support
- Closely examine the patient to elucidate the cause of their illness
- If
deterioration occurs, control airway with an advanced airway following
the difficult airway algorithm
- USE DOUBLE SET UP METHOD
- If not present, proceed to step two
- If present,
do the following:
- Examine the
oropharynx to determine if pharyngitis present
- If yes, provide symptomatic treatment and consider antibiotics if severely ill or if practicing in an endemic setting of rheumatic fever
- If not:
- Look for a
mass (e.g., PTA, tongue elevation, angioedema)
- If present, provide disease-focused therapies and consult ENT/Anesthesiology for airway and surgical support if needed
- If not
present, consider:
- Nasopharyngoscopy
- Advanced imaging
- Empirical treatment for epiglottitis, if suspected, prior to imaging
- Look for a
mass (e.g., PTA, tongue elevation, angioedema)
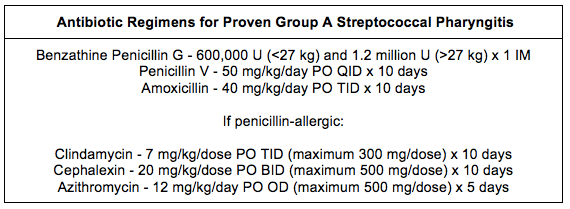
[7] What antibiotics can be used in the patient with suspected or confirmed streptococcal pharyngitis? [Box 20.2]
The list below outlines the available antibiotic agents for the patient with proven GAS pharyngitis. It is adapted from Box 20.2 – Antibiotic Regimens for Proven Group A Streptococcal Pharyngitis in Rosen’s 9th Edition. Please refer to this table for further detail.
WiseCracks:
[bg_faq_start][1] In what age groups is streptococcal pharyngitis rarely seen?
Answer:
Remember, streptococcal pharyngitis is exceedingly rare in persons <3 years of age
Additionally, persons 45 years of age or older are unlikely to have streptococcal pharyngitis
[2] What is Waldeyer’s Tonsillar Ring?
Answer:
Waldeyer’s tonsillar ring or the pharyngeal lymphoid ring consists of the following:
- Adenoids (also referred to as the pharyngeal tonsils)
- Tubal tonsils
- Palatine tonsils
- Lingual tonsils
[3] What is the “thumb sign” and what pathology does it point to?
Answer:
The thumb sign on lateral neck X ray demonstrates widening of the epiglottic silhouette. Likely indicates EPIGLOTTITIS. See Figure 20.2 to get better idea of the radiographic finding.
[bg_faq_end]Uploaded and copyedited by Ryan Fyfe-Brown

Dillan Radomske
Latest posts by Dillan Radomske (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021

Owen Scheirer
Latest posts by Owen Scheirer (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021