

This updated episode of CRACKCast covers Rosen’s Chapter 017, Headache (9th Ed.). Headache is an exceedingly common ED presentation with a multitude of possible causes. This podcast will help you to keep your differentials broad by breaking down the not so bad, the bad and the ugly of headaches.
Shownotes – PDF here
[bg_faq_start]Rosen’s in Perspective
Alright, y’all – let’s get back into another episode of CRACKCast with another headache provoking case:
You are working the night shift at a community ED when you pick up a chart of a 36-year-old female who has been waiting for the last four hours. The presenting complaint states “Headache – severe”. You ask if you can get this patient into a room quickly, but you are met with some pushback from your colleagues. The triage nurse tells you they see this patient as a “frequent flyer” for “migraines” about once every two weeks. Her vitals were normal on the triage form, so she was triaged a CTAS 3. When you finally get a place to see her, she is somewhat confused and is complaining of a 10/10 headache. It is difficult to get much of a history out of her given her depressed LOC. There are no focal findings on her exam. Suddenly, she starts to seize – what do you do?
As you may have guessed, today we are covering Chapter 17 in Rosen’s 9th Edition – Headache. The case above is designed to highlight a few key points we wanted to make in this RIP section. First – headache is an exceedingly common cause of presentation to the ED. Second, just because people have a primary headache disorder does not mean we can attribute every headache they are having to the disorder aforementioned. Third, if a patient presents with focal findings, altered LOC, or signs/symptoms of systemic illness in the setting of a headache, DIG FOR THE BAD STUFF. While most people presenting with headache have benign causes of their complaint, others will harbor sinister pathology that needs to be sought out.
We will cover it all on CRACKCast today. We will discuss the good, the bad, and the ugly. We will go over the cannot-miss diagnoses for headache, the utility of neuroimaging and lumbar puncture (LP) in patients presenting with headache, and how to perform those all-too-complicated physical exam maneuvers that you will be pimped on during your next Neurology rotation. So, sit back, sip your coffee, and listen away!
[bg_faq_end]Core Questions:
[bg_faq_start][1] List three primary headache disorders
While there are many types of primary headache disorders, there are three that steal the show, so to speak. These are listed below:
- Tension-type headache
- Typically has the following symptom profile:
- Lasts 30 minutes to 7 days
- Bilateral location
- Pressing or tightening (non-pulsatile) character
- Mild to moderate intensity
- No aggravation by activities
- No nausea/vomiting
- No photo/phonophobia
- Typically has the following symptom profile:
- Migraine headache
- Typically has the following symptom profile:
- Lasts for 4-72 hrs
- Unilateral
- Throbbing or pulsatile in nature
- Accompanied by photo/phonophobia
- Accompanied by nausea +/- vomiting
- Can be associated with aura
- Often aggravated by activities (e.g. walking)
- Typically has the following symptom profile:
- Cluster headache
- Typically has the following symptom profile:
- Stabbing or boring-type pain
- SEVERE intensity
- Lasts 15-180 minutes
- Typically, pain centered around the eye or temple
- Ipsilateral autonomic features (facial sweating, conjunctival injection, nasal congestion, rhinorrhea, ptosis, miosis)
- Sense of restlessness or agitation
- Typically has the following symptom profile:
Based on population-based data, tension or tension-type headaches are the most common primary headache disorder. Migraines are similarly common, but are more likely to send people to the ED. Cluster headaches, an exceedingly debilitating form of brain-cruncher, are uncommon, but when present cause a tremendous amount of grief for our patients.
[2] Describe the pathophysiology of migraines and name three Emergency Department treatments for same
The understanding of migraine pathophysiology has changed markedly over the last several years. While once thought to be the result of CNS vascular changes, migraines are now thought to be caused by primary neuronal dysfunction that result in the symptoms of migraine headaches. Cortical spreading depression leading to a propagating wave of neuronal depolarization that extend across the cerebral cortex are now thought to be the cause of migraines. This spreading cortical depression is thought to cause the migraine aura and activation of trigeminal nerve afferents (causing inflammatory changes in the meninges and thus the pain associated with migraines). There are also changes in the blood-brain barrier caused by this neuronal dysfunction that further contribute to migraine symptoms.
As for ED treatment (i.e. for people with moderate to severe migraines), you have the following options:
Strong Evidence-based Treatments:
- Sumatriptan 6 mg SC
- Note: difficult to give in ED – ++ contraindications
- Antiemetics (both antiemetic agents and help to provide pain relief)
- Metoclopramide 10 mg IV
- Prochlorperazine 10 mg IV or IM
- Chlorpromazine 0.1 mg/kg IV to a total dose of 25 mg IV
- ***when giving antiemetics, consider giving diphenhydramine 12.5-25 mg IV q1h x2 to prevent akathisia or dystonic reaction – not great evidence, but consider it
- Ketorolac 30mg IV or 60 mg IM
- Acetaminophen PO
- Dexamethasone 10-25 mg IV to reduce rates of early migraine recurrence
Weak Evidence-based Treatments:
- IV MgSO4
- Dihydroergotamine 1 mg IV combined 10 mg IV
- Occipital nerve blocks
- Sphenopalatine nerve blocks
- Subdissociative dose ketamine
- IV Propofol
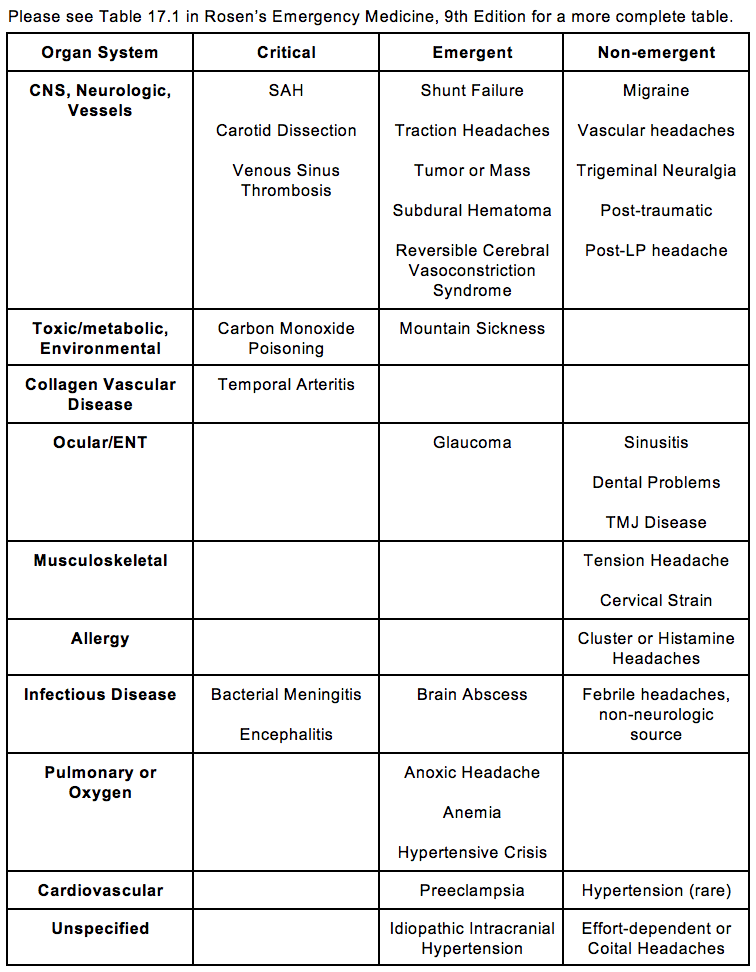
[3] List five critical and five emergent causes of headache (Table 17.1)
[4] Outline your approach to the history for the patient presenting with headache (Box 17.1)
Approach to the History:
While taking the patient’s history, it becomes important to do what they taught you in medical school. Start broad, and do not anchor too quickly. In the context of a busy ED, it is easy to fall into the trap of seeing every headache as a migraine. While you will often be correct, you will miss the dangerous things lurking about.
Our approach that we present here closely mirrors the approach presented in Rosen’s. We tailor our history to hunt for the diagnoses that could potentially kill the patient, while also looking for confirmatory historical data that lead us to the diagnosis of more benign conditions. Our approach is as follows:
- Determine the onset of pain
- Ask about thunderclap pattern headaches (sudden onset, worst headache they have ever had)
- Determine the patient’s activities at the time of headache onset
- If they patient was able to detail the exact moment when their headache came on, this could indicate that the patient has a potentially serious cause of their headache (e.g., SAH)
- Ask about physical activity just before their headache, as this is more likely to suggest a vascular cause
- Ask about coital activities, as this has been associated with SAH and coital headaches
- Inquire specifically about any trauma incurred by the patient
- Suss out the intensity of the pain
- This will not necessarily help you make the diagnosis, but it will give you a gauge as to treatment efficacy later on in the encounter
- Remember that rapid resolution of pain does not exclude a serious cause of their headache
- Elicit the character and location of the pain
- This will help you differentiate between different types of headache
- Determine the exacerbating and relieving factors for the pain
- Consider the environment in which the pain arose. This will help you determine if there may have been exposure to CO
- Most other serious causes of pain will not be rapidly alleviated before ED treatments are initiated, so keep this in mind
- Inquire as to other associated symptoms on a full review of systems
- Determine what, if any, history of headache they have had
- This will allow you to determine if this headache is like their previous headaches. Any deviation from their normal pattern and intensity warrants careful investigation
- If the patient has had neuroimaging recently, you plan for investigation may change, so look back in their old chart/EMR
Box 17.1 in Rosen’s 9th Edition gives us a solid list to keep in mind the next time you pick up the headache chart. It is entitled “Emergent Causes of Headache and Associated Risk Factors” and gives you the tools you will need to further tailor your history to look for those persons at higher risk for malignant causes of their headache. Learn it, use it, love it.
We have included an abbreviated version of the box here. For a more complete version of the chart, please refer to Rosen’s 9th Edition.
Box 17.1 – Emergent Causes of Headache and Associated Risk Factors
- Carbon Monoxide Poisoning
- Breathing in enclosed or confined spaces with engine exhaust or ventilation of heating equipment
- Multiple household members with the same symptoms
- Wintertime and working around machinery or equipment producing carbon monoxide (e.g., furnaces)
- Meningitis, Encephalitis, Abscess
- History of sinus or ear infection or recent surgical procedure
- Immunocompromised state
- General debilitation with decreased immunologic system function
- Acute febrile illness – any type
- Extremes of age
- Impacted living conditions (e.g., military barracks, college dormitories)
- Lack of primary immunization
- Temporal Arteritis
- Age >50
- Females > males (4:1)
- History of other collagen vascular disease (e.g., SLE)
- Previous chronic meningitis
- Previous chronic illness, such as TB, parasitic, or fungal infections
- Glaucoma – acute angle closure
- Not associated with any usual or customary headache patterns
- History of previous glaucoma
- Age >30
- History of pain in a dark environment
- Increased intracranial pressure
- History of previous benign intracranial hypertension
- Presence of CSF shunt
- History of congenital brain or skull abnormalities
- Female gender
- Obesity
- Cerebral Venous Sinus Thrombosis
- Female gender
- Pregnancy, peripartum, hormone replacement therapy or OCP use
- Prothrombotic conditions
- Reversible Cerebral Vasoconstriction Syndrome
- Episodic severe pain, with or without focal neurological findings or seizure
- Recurrent episodes over a period of several weeks
- Exposure to adrenergic or serotonergic drugs
- Postpartum state
- Intracranial Hemorrhage
- SAH
- Sudden severe pain
- Acute severe pain after sexual intercourse or exertion
- History of SAH or cerebral aneurysm
- History of polycystic kidney disease
- Family history of SAH
- Hypertension – severe
- Previous vascular lesions in other areas of the body
- Young and middle-aged
- Subdural Hematoma
- History of alcohol dependency with or without trauma
- Current use of anticoagulation
- Epidural Hematoma
- Traumatic injury
- Lucid mentation followed by acute altered mentation or somnolenceAnisocoria on physical examination
- SAH
[5] Outline your approach to the physical exam for the patient presenting with headache (Table 17.3)
Approach to the Physical Exam:
As you may expect, doing a thorough neurological examination is key. Performing an in-depth cranial nerve examination is essential, as you may only elicit focal deficits or abnormalities on this portion of the exam.
Performing a good HEENT exam is also essential, as this may give you diagnostic clues as to what is causing the patient’s headache (e.g. signs of basal skull fracture, sinus pain, ocular findings suggesting acute angle-closure glaucoma). Looking for signs of meningismus is also key here.
In addition to the examinations aforementioned, use your review of systems to guide the remainder of your exam.
Table 17.4 in Rosen’s 9th Edition titled “Diagnostic Findings in Emergent Causes of Headache” gives us a good list of things to look for when examining patients with headache. An abbreviated version is provided below.

[6] Describe your diagnostic approach to the patient with a suspected SAH
So, you go to see a patient who you suspect has suffered a subarachnoid hemorrhage. The time is ticking, so let’s get kicking.
There is a great CanadiEM article that articulates the work-up necessary to rule in or rule out a SAH in your patients with thunderclap headaches. We have listed the link below: https://canadiem.org/subarachnoid-hemorrhage/
Determining the time of onset of the headache is EXCEEDINGLY IMPORTANT. The window in which CT can be relied upon to rule out SAH is 6 hours. So, work that out.
If the patient has a negative CT scan for SAH (as determined by a qualified radiologist) AND symptom onset has been within 6 hours, you can accurately state that the patient’s headache has not been caused by SAH.
If the patient falls outside of the 6 hour window, you will have to go a little bit further. You will need to do an LP to look for signs of bleeding into the CSF. You are looking for the following:
- Increased opening pressures
- Blood in the CSF that does not clear from tubes 1 to 4
- Xanthochromia (yellow or pink tint to CSF)
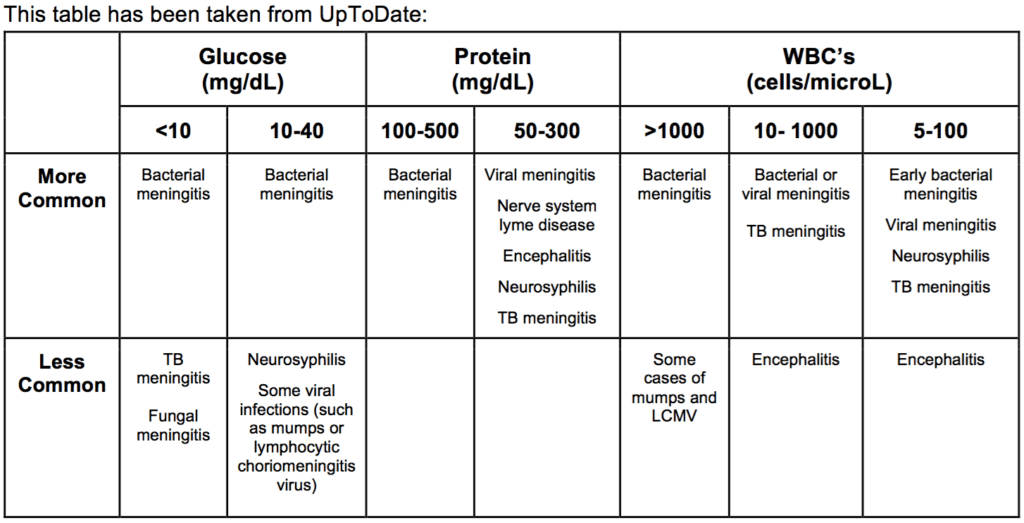
[7] Detail the findings on LP that would suggest your patient has bacterial meningitis
WiseCracks:
[bg_faq_start][1] What percentage of patients presenting with headache to the ED have a SAH?
Despite how much we have spoken about SAH’s today, they are actually quite rare. According to Rosen’s Emergency Medicine, only 0.5-6% of patients with acute headache in the ED have this pathology.
The reason we have spoken so much about it is because it is frequently misdiagnosed in the ED. Rosen’s quotes that SAH is misdiagnosed in over 25% of cases. So, when a person presents with the following, always have SAH high on your DDx:
- Thunderclap headache
- Headache + loss of consciousness
- Severe headache with neck stiffness/pain
- Onset of headache during exertion
- Age >/40 years
- Limited neck flexion on ROM
[2] Outline the SNOOP MEETS Pregnancy mnemonic
Another CanadiEM gem coming at you. This mnemonic will help you focus your histories to look for red flags of secondary causes of headache. It can be found here: https://canadiem.org/tiny-tips-snoop-meets-pregnancy-headache-mnemonic/
Systemic symptoms – fevers, chills, night sweats, protracted vomiting
Neurological signs that are focal, altered LOC, seizures
Onset abrupt or sudden
Old age (>50 Y)
Progression or pattern change
Morning worse
Exertion/posture/sexual activity worsens headache
Exposure Hx
Trauma
Secondary risk factors (i.e., CA, HIV)
Pregnancy
[3] Which diagnostic test is best to establish the diagnosis of cerebral venous thrombosis?
Answer: MR Venography
MR Venography is the preferred method of diagnosis. CT venography can be used as an alternative to imaging if MR venography is not available. CT alone is unreliable in detecting cerebral venous thrombosis, and is negative in up to 30% of cases.
[4] Detail how to elicit Kernig’s and Brudzinski’s Sign
Kernig’s Sign
Position the patient supine. Next, place the hips in 90 degrees of flexion. Once in this position, attempt to passively extend the knee. A positive Kernig’s sign is noted when there is resistance to extension of the knee >135 degrees OR if there is a pain in the posterior thigh and/or the lower back
Brudzinski’s Sign
Position the patient in supine. Next, flex the chin to the chest. A positive Brudzinski’s sign occurs when flexing the chin to the chest causes the patient to flex their knees and hips.
So, aside from scoring you bonus points with Neurology off-service, what good are these tests going to do you? Long-and-short, they are going to do help you out a decent bit. One study found that for patients with severe meningeal inflammation, they have roughly a 5% sensitivity, and a 95% specificity.
[bg_faq_end]Uploaded and copyedited by Chloe LaBrie.

Dillan Radomske
Latest posts by Dillan Radomske (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021

Owen Scheirer
Latest posts by Owen Scheirer (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021