

This episode of CRACKCast covers Rosen’s Chapter 51, Wrist and Forearm Injuries. These common injuries have multiple eponyms, but this podcast helps deliver the fundamental approaches needed for management for these recurrent patterns of injury.
Shownotes – Link to PDF Here
[bg_faq_start]Rosen’s in Perspective
[bg_faq_start]What is the wrist?
Distal radius/ulna → CMC junctions
- 8 carpal bones in two rows of four
- Bones: SLTPTTCH
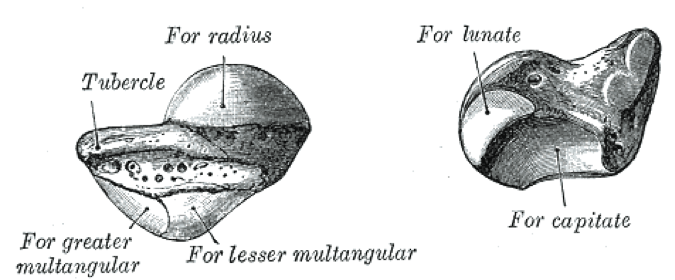
- The Radius has three articular surfaces:
- Radiocarpal joint
- Distal radial ulnar joint (DRUJ)
- Triangular fibrocartilage complex (TFCC).
- Only the radius actually interfaces with the carpi – scaphoid and lunate
- The ulna is separated from the carpals by the TFCC
- This binds the radius, ulna, lunate, and triquetrum together
- The DRUJ is a “synovial pivot” where the distal radius articulates and rotates on the fixed ulna. This movement is stabilized by the TFCC
- All the carpals (except pisiform which is embedded in FCU) are contained in a synovial capsule.
- Their movement is passive based on what the metacarpals, radius and ulna do
Wrist ligaments:
- Intrinsic ligaments – connect the carpal bones
- Eg. scapholunate & lunotriquetral ligaments
- Extrinsic ligaments – link the carpal bones to the distal radius, ulna, and metacarpals
- Eg. the volar proximal and distal arcades
- Eg. the dorsal extrinsics
Vascular supply
Radial and ulnar arteries
- **The intrinsic blood supply of the carpal bones enters distally to proximally in most cases**
- Especially: scaphoid, capitate, lunate:
- Each of these have a single distal vessel giving them their blood supply
- Especially: scaphoid, capitate, lunate:
Nerves
- Radial and ulnar nerves have dorsal branches which cross the dorsum of the wrist at each respective styloid
- The Median nerve is all volarly located: crosses radial and deep to the palmaris longus tendon
- The ulnar nerve lies within Guyon’s canal – between the pisiform and the hook of the hamate. [fig 51-3
- Why is the wrist important?
- Many movements, including circumduction
- How to examine the hand?
- See Table 51-1 or listen to episode 50
- Clinical features of wrist injury
- History
- Mechanism of injury!
- Full detailed hx
- Physical Exam
- Compare to the normal wrist
- Find the point of maximal pain
- Dorsal structures:
- Describe it in relation to known landmarks: ulnar styloid, radial styloid, snuff box, lister’s tubercle (on the radius) – proximal to scapholunate – and a point for wrist arthrocentesis.
- Also where the lunate shows up with volar flexion
- Ulnar to this is the DRUJ and the triquetrum
- Volar structures:
- Scaphoid tubercle is distal to the radial styloid
- Pisiform is distal to the ulnar styloid (by the hypothenars)
- Distal and radial to the pisiform is the hook of the hamate
- Nerve and vascular exam
- Dorsal structures:
- History
1) Describe normal radiographic relationships:
- Should get these views:
- PA, lateral, oblique
- Anatomy to identify: the ulnar styloid, the extensor carpi ulnaris groove
- There are TONS of other views
- Eg. clenched fist view, scaphoid views, carpal tunnel views, reverse supinated view
- See table 51-2 for more details
- PA, lateral, oblique

Radial length measurement
- The radial styloid process should extend beyond the end of the articular surface of the ulna by 9 – 12 mm on a PA radiograph
Figure 51-4

- There may be some degree of ulnar variance that affects this distance on the PA view due to wrist rotation/flex/ext/variation/injury
- Positive ulnar variance:
- Ulnar articulation is more distal (+ve) = the ulna is moved distally. As in ulnar impaction/abutment syndrome. Found in TFCC injury
- Neutral = 9-12mm = NORMAL
- Negative ulnar variance:
- The ulna has moved “away” (-ve) from the carpals or proximally. E.g. Kienboch’s disease of the lunate.
- Positive ulnar variance:
Radial inclination
Aka: ulnar slant
The articular surface of the radius on a PA view angle normally is 15-25 degrees – sloping towards the ulna
Volar Tilt
The distal radius on a lateral view X-ray should have 10-25 degrees of volar tilt. [See Fig 51-6]

1) To make sure it is an adequate lateral view: How to know if it is an adequate lateral view?
2) The distal radius should line up with the lunate, capitate, and the 3rd metacarpal
- Forming three C-shapes, and the convexity of the distal capitate < 10 degrees
- See [fig 51-8]

3) Finally, the scapholunate angle should be 30-60 degrees and the capitolunate angle should be 0-30 degrees [fig 51-9]

- If any of these 3 measurements are off consider carpal ligament injuries and carpal instability
- See below about DISI and VISI
Scapholunate angle
- See Fig 51-9 as we explain it on the podcast.
- Longitudinal axis of the scaphoid and lunate
Capitolunate angle
- See Fig 51-9 as we explain it on the podcast.
- Intersection of the capitate and lunate central axes.
Wrist arcs
- Carpal bones on the PA view should only have 1-2 mm between each of them. With parallelism
- On the PA radiograph smooth lines (Gilula’s lines or carpal lines) can drawn like arcs along the articular surfaces.
- disruption = ligament/instability/#
Take home: memory aids: 22 volar tilt – 22 radial inclination – 11 radial length – 1-2 mm carpal bone spacing.
- Just remembers 1”s and 2”s in some combination.
2) Describe X-Ray findings and management of:
[bg_faq_start]Scaphoid fracture
Most commonly #’d carpal bone (15-40 yr. Olds with a FOOSH), high complication rate
- (5-40%) of AVN/non-union
- Anatomy:
- 1) tuberosity and distal pole
- 2) waist
- 3) proximal pole
Physical exam:
- Dorsal wrist pain – distal to radius
- Limited ROM of wrist and thumb
- Snuffbox tenderness and swelling
- Detection may increase with radial OR ulnar deviation*
- Watson’s scaphoid shift test
- Axial compression of the 1st MC*
- Pain on thumb/index finger pinch
- Palpation of the scaphoid tubercle volarly*
X-ray findings:
- 15% of plain radiographs immediately after the fall miss the injury
- Need to get scaphoid views to increase sensitivity
- Findings:
- Fracture lucency, obliteration of the scaphoid fat pad
Optimal imaging?
- “Still controversial”, but definitely not bone scans
- CT: 93% sensitive for occult fracture identification acutely
- MRI: “100%” sensitive
Treatment:
- Anyone with the suspicion of scaphoid #’s needs immobilization, and repeat imaging in 7-10 days
- Uncomplicated, non-displaced #s
- Immobilization in thumb spica cast for 6-12 weeks
- If short arm casting: wrist in 10 deg. Flexion, mild radial deviation, thumb IP free
- **some people put a long arm cast for the first 1-2 weeks**[2]
- **the more proximal the fracture the higher the risk of AVN and non-union**
- Because blood flows distal to proximal through the scaphoid tuberosity
- “Urgent” referral for surgical fixation in cases:
- “Unstable”, displaced > 1mm, other associated #s. Increased S-L/C-L angles
- Immobilization in thumb spica cast for 6-12 weeks
Lunate fracture
- Rare
- Common in people with congenitally short ulna
- FOOSH injury with extreme dorsiflexion
- Px: dorsal wrist pain, pain with axial loading of long finger, tenderness distal to Lister’s tubercle.
- Risks of carpal instability, AVN, nonunion, Kienbock’s disease
Imaging & management:
- Difficult to see on plain films, should any suspected fracture should be managed as a scaphoid # with a thumb spica cast with follow up in 7-10 days
- Any displaced fracture should be reduced, then with ortho referral
- All need hand surgeon expert for long term management and complications
Triquetral fracture
Second highest risk of # after the scaphoid.
- FOOSH injuries or blow to the hand
- Associated with perilunate and lunate dislocations***
- Physical exam shows pain distal to the ulnar styloid
- LOOK for minimally displaced triquetral avulsion fractures or dorsal chip fractures on the lateral view
- Body fractures may be seen on the AP view
Treatment:
- Short arm splint or ulnar gutter with f/u in 1-2 weeks
- The definitively treated in short arm cast 4-6 weeks
DID: If pain persists → immobilize in a thumb spica with follow-up.
- Many argue for CT and/or MRI imaging sooner than later, especially for scaphoid #’s.
[bg_faq_end] [bg_faq_end][bg_faq_start]
3) Describe Mayfield’s stages of carpal instability
- These occur in people with FOOSH injuries
- Dorsal swelling and wrist pain
- Limited wrist ROM
- Physical exam shows:
- Dorsal wrist pain – at the scapholunate ligament
- Watson’s scaphoid shift test producing clunks or snaps when moving the wrist from ulnar to radially
- Not useful acutely!
- Typically stages 2-4 have visible wrist deformities and median nerve sensory loss
- Watson’s scaphoid shift test producing clunks or snaps when moving the wrist from ulnar to radially
- Dorsal wrist pain – at the scapholunate ligament
Figure 51-20

- The LUNATE is the centre of attention
- The sequential stages of carpal instability – shows an intercarpal ligament injury proceeding from the scapholunate inter-space then distally to the capitate then to the triquetral then to the radio-carpal space.
- Each stage may be associated with an adjacent carpal bone #
- Caused by carpal hyperextension, ulnar deviation and inter-carpal supination.
- Stage 1: scapholunate dissociation
- PA view showing the “terry thomas sign” – front teeth gap
- Aka: Maddona sign, David letterman
- Due to scaphoid rotary subluxation
- Also may show the “signet ring sign” where the scaphoid is seen end on
- ****scapholunate dissociation may NOT be seen on routine radiographs, despite clinical suspicion
- So stress views (clenched fist in ulnar deviation) may show pathologic > 3 mm scapholunate gap
- PA view showing the “terry thomas sign” – front teeth gap
Figure 51-21

- Stage 2: Perilunate dislocation
- On the lateral view the lunate articulates with the distal radius, but the capitate is dorsally dislocated
- The PA view shows overlap of the distal and proximal carpal rows (abnormal carpal arcs!)
- **don’t miss associated scaphoid, radial styloid, capitate #’s**
- Key on the lateral radiograph = the lunate maintains its articular connection and alignment with the radius
- Stage 3: perilunate dislocation WITH triquetrum dislocation
- Same as stage 2, except the triquetrum is dislocated
- Need the PA view to see it – to see carpal overlap of the triquetrum with the lunate/hamate
- May also have volar lunate #
- Stage 4: lunate dislocation
- “Triangular lunate” and no articulation with the radius
- Aka: “piece of pie sign”
- “Spilled tea-cup sign on the lateral view” – where the lunate has been dislocated volarly
- the capitate shifts posterior to the lunate and may contact the distal radius
- “Triangular lunate” and no articulation with the radius
Complications:
- Median nerve injury, chronic instability → arthritis
Diagnosis:
- MRI (Only 63% sens, and 86% sensitivity for scapholunate injury)
- Arthroscopy = gold standard
ALL need urgent orthopedic/plastics consultation for reduction/pinning/repair
Pirates of the carribean: “Mayfield tripped and FOOSHed while he was watching a lunar eclipse with Sgarbossa, Captain Jack and pieces of his raiding pirate crew”
4) Describe DISI and VISI
These refer to carpal ligament instability – leading to altered wrist kinematics. Broad types of wrist ligament injuries include: “midcarpal instability” (MCI), dorsal intercalated instability (DISI), or volar intercalated instability (VISI), and radiocarpal instability.
They usually present with people complaining of chronic wrist pain, weakness, limited ROM, and wrist clicking.
- wrist pain dorsally or volarly – @ scapholunate/lunotriquetral joints
- asymmetric wrist appearance
Hx risk factors:
- Kienbock’s disease
- Rheumatoid arthritis
- Congenital carpal ligamentous instability
Anatomy review:
- Midcarpal joint – at the distal and proximal carpal bone rows
- Intercalated segment = proximal row of carpal bones (this row moves passively with NO muscular attachments)
Figure 54-24 for the hardcore keeners who want to measure angles and show off trigonometry
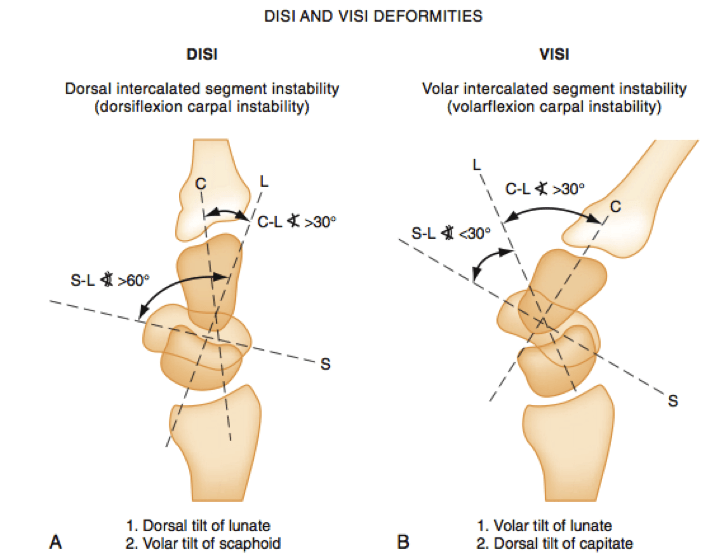
DISI
- The lunate is tilted dorsally
- An increase in scapholunate and capitolunate angles
- More common than VISI
- May occur in any peri lunate or scaphoid pathology
VISI
- The lunate is tilted volarly
- A decrease in the scapholunate angles, and an INCREASE capitolunate angle.
- Occurs after lunotriquetral or triquetrohamate joint injury
Diagnosis:
- X-Ray (lateral views)
- CT
- MRI, video-wrist fluoroscopy
Treatment: complicated, controversial surgical approaches
Dumb it down: find the lunate, see if it is tilted volarly or dorsally, pick up the phone, go home.
5) Describe x-ray findings and management of:
The distal radius and ulna injuries are very common!
- Women > 50 yrs have a 15% lifetime risk of these injuries!
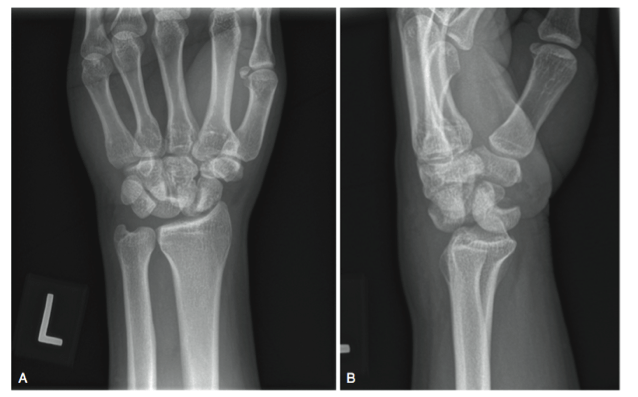
Colles’
- Most common wrist #
- Transverse # of the distal radial metaphysis, with dorsal displacement and angulation.
- May have associated extension, comminution, intra-articular extension, and up to 60% have an ulnar styloid #
- Causes the “dinner fork deformity” on physical exam
- Xrays show:
- Potential extension into the DRUJ, dorsal displacement and angulation, loss of normal volar tilt.
- Treatment:
- An early anatomic reduction with restoration of radial length, correction of dorsal angulation to normal volar tilt (or at least neutral).
- Reasons for emergent reduction:
- Neurovascular compromise, soft tissue tension.
- Urgent reduction:
- Loss of volar tilt on lateral view (>10 deg dorsal angulation)
- Radial shortening or +ve ulnar variance > 2mm
- Inadequate reduction is common in cases of:
- intra-articular fragments, radial inclination <15 deg,
- Immediate ortho referral for:
- Unsuccessful closed reduction, neurovasc. Compromise, compartment syndrome, open #s.
- Complications:
- Loss of function, median nerve injury, cast complications, acute carpal tunnel syndrome.
- Transverse # of the distal radial metaphysis, with dorsal displacement and angulation.
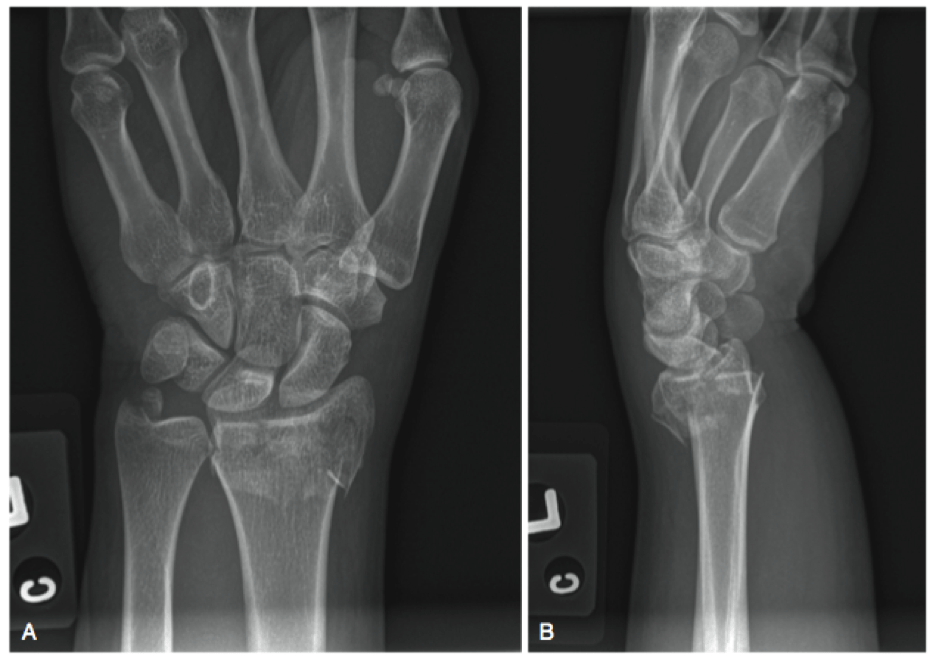
Smith’s
- “Transverse # of the metaphysis of the distal radius with volar displacement and angulation.”
- May extend in any direction
- Mechanism:
- Blow to dorsal wrist, fall onto dorsum of hand (extreme plamar flexion), fall backwards (FBOOSH) in supination
- Lateral view on x-ray is key
Treatment: reduction to normal radial anatomy, immobilization. MORE likely to need operative fixation due to instability. MORE likely to have associated neurovascular compromise of median nerve than the Colles fracture. Ortho follow-up.
Finger trap technique for distal radius #s: patient supine, with the elbow at 90 degrees of flexion and 10 pounds of weight for ten minutes before a reduction attempt.
Barton’s
- See fig 51-29
- Oblique intra-articular fracture of the rim of the radius (look at the lateral view) with carpus dislocation
- The dorsal or volar rim can be displaced
- Rare, high velocity injuries
- Urgent ortho consultation for reduction/stabilization (unstable!)

Hutchinson’s / Chauffer’s
- Intra-articular fracture of the radial styloid
- Look on the PA view for a transverse fracture of the radial metaphysis with extension through the radial styloid into the radiocarpal joint
- Needs reduction → CRUCIAL to have perfect reduction given the location of all the wrist ligaments on the radius such as the scapholunate ligaments
- Sugar-tong splint → short arm cast
DRUJ Disruption
- Can occur isolated or with any radius injury (see below)
- Difficult to diagnose, especially if it is in isolation, with most radiographs being falsely normal
- And clinical findings may be the only clue
- Usually FOOSH mechanism, or rapid twist due to machinery (with TFCC injury)
- Px:
- Crepitus/pain of DRUJ on pronation and supination
- Compare both sides and look for changes in the ulnar styloid position
- Dx:
- Lateral view of ulna with >20 degrees of angulation
- Fracture of ulnar styloid base
- Must rule out the essex-lopresti syndrome!
- PA view may show > 2mm of widening or overlap
- CT much more accurate
- Treatment:
- Ortho
- Closed reduction with long arm cast and wrist in supination
- May need operative ORIF or CRIF
6) Describe management of the following pediatric fractures:
- Pediatric distal radius #s:
- Two main types:
- Involving the growth plate
- Involve BOTH cortices of bone, use SALTER system to classify
- Usually need reduction, but are often unstable and at risk for compartment syndrome
- Need ortho follow up and investigation for other injuries
- Short arm splint
- Involving the radial metaphysis:
- Greenstick
- Torus
- Complete fractures
- Involving the growth plate
- Two main types:
Forearm fractures
- More than ½ of all pediatric #s
- Three types:
- Greenstick
- One cortex is disrupted
- Complete
- Need reduction, ortho consultation, and follow-up in a long arm cast
- Plastic deformation
- See figure 51-43
- Traumatic bowing without any break in the cortex
- Usually need ortho consultation and advice
- Rules of thumb:
- “10 degrees of angulation, in a child < 10 yrs, is ok” – the bone should remodel well without reduction
Torus fractures
- Most common.
- Buckle of the radial cortex [fig 51-32]
- No actual widening of the cortex
- Treatment:
- Short arm splint and ortho follow-up in 2-3 weeks
- All heal and remodel well

Greenstick fractures
- Incomplete metaphyseal fractures outside the growth plate
- Disruption of the cortex on one side and angulation and bowing of the opposite side [fig 51-33]
- Usually need reduction if angulation is > 10 degrees
- Treated with short arm splint with ortho follow-up
7) List 8 RFs for Carpal Tunnel Syndrome + Describe 2 tests for CTS
- Let’s review some anatomy of the carpal tunnel:
- All the flexors of the digits (9), median nerve slide under the flexor retinaculum (which is an arch – transverse carpal ligament – that goes from the scaphoid to the pisiform)
- The flexor carpi radialis lies outside the carpal tunnel.
- CTS is the most common entrapment
- Median nerve
- Don’t forget about ACUTE CTS
- Usually traumatic, hemorrhagic, infectious, related to carpal dislocations, etc.
Risk factors
- Female – pregnancy or menopause
- RA
- Hypothyroidism
- Connective tissue disease / collagen vascular disease
- Diabetes
- Renal failure
- CHF
- Distal radius #
- Repetitive hand flexion activities
Physical exam:
- Must do a chest, neck exam to detect referred symptoms
- Phalen’s
- 76% sensitivity, and 80% spec.
- Flex wrists with forearms horizontal for 60 seconds,
- +ve if paresthesias or numbness develops in the median nerve distribution
- Tinel’s sign
- Sens 42-85%
- Tapping on the median nerve with symptoms
- Durkans test
- Sensitivity 87%, spec 80%
- Direct median nerve compression
Gold standard: nerve conduction studies (85-90% sens)
8) Describe the Monteggia and Galeazzi’s fracture patterns
- Essential to include wrist and elbow views!
Monteggia
- “A fracture dislocation: the #’d ulnar diaphysis, with anterior dislocation of the radial head”
- MURG
At high risk for posterior interosseous nerve injury (paralysis or weakness of finger and thumb extension)
***don’t miss the subtle radial head subluxation!!***
- Draw the radiocapitellar line to be sure (on all views)
Adults need ORIF
Kids can usually have a long arm cast with the arm in supination
Galeazzi’s
- “A fracture dislocation: the #’d distal ⅓ of the radius, with a dislocation of the DRUJ”
- GRUM
From FOOSH or MVC
- Key is not to miss the DRUJ injury – because it may not be seen on x-ray and only subtly present on physical exam
- > 2mm space between radius and ulna, with possible radial shortening = concerning!
All adults need surgical fixation, because this is an unstable injury even if successfully reduced. Kids can usually get away with a long arm cast.
Wisecracks
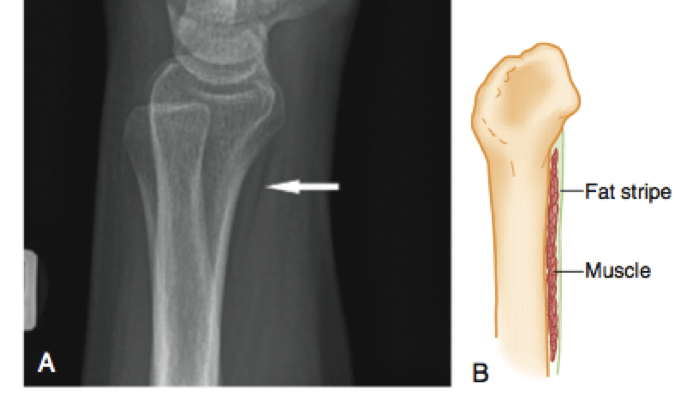
What is the pronator quadratus fat pad?
- See fig 51-10
- A normal fat stripe on the lateral wrist view, which if obliterated, absent or displaced can herald wrist disease (SSTI’s, inflammatory conditions, hematomas, or occult #s)
- Poor sensitivity
Extra fractures not covered in the podcast:
- Hamate #s
- Can be palpated 1 cm distal and radial to the pisiform volarly
- Fractures are rare, but usually involve the hook of the hamate
- X-rays are poorly sensitive even with special views
- CT!
- Hook fractures can lead to little finger flexor tendon rupture, neuropraxia, or vascular compromise
- Should be casted in a thumb spica with f/u
- Many may need ORIF/excision
- Pisiform #s
- Lies in the FCU tendon, and rarely fractured
- Carry high risk of ulnar nerve injury and vascular compromise
- Need special x-ray views or CT/MRI
- Good prognosis with short arm cast x 4 weeks.
- Trapezium #s
- Rare
- Poorly visualized with xrays
- Thumb spica
- May need ORIF for displacement of CMC involvement
- Capitate #s
- Rare
- Risk of AVN
- Most seen on x-ray
- Thumb spica and follow-up
- Trapezoid #s
- Rare, usually with other carpal injuries
- Need special oblique views for better visualization
- Thumb spica and follow up
- Essex-Lopresti lesion
- Longitudinal radio-ulnar disassociation
- Triad of: disruption of the forearm interosseous membrane, radial head injury/#, and DRUJ violation
- Very elusive diagnosis, with some non-stress x-rays being normal
- MRI and/or ultrasound needed to make the diagnosis
- Longitudinal radio-ulnar disassociation
- Ulna fractures:
- Carefully look for open! Fractures
- Look for associated PRUJ or DRUJ injuries
- At very high risk for being unstable
- Compartment syndrome
- Common in forearm fractures
- Diagnosis:
- > 30 mmHg compartment pressure
- Within 20 mmHg of the diastolic pressure
- Can affect one of the three compartments – volar, mobile (lateral to the radius), dorsal.
- Adults – distal radius fracture highest risk
- Children – supracondylar fractures highest risk
- Resulting in Volkmann’s ischemic contracture of the hand and wrist
- Diagnosis:
- Common in forearm fractures
This post was uploaded and copyedited by Riley Golby (@RileyJGolby)
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018

Adam Thomas
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018