

Today’s podcast review Chapter 37 in Rosen’s 9th Edition and gives you the tools you will need to manage your next case of neck trauma in the ED.
[bg_faq_start]
Rosen’s In Perspective
Alright podcast listeners, let’s get into another episode of CRACKCast. Today we will start out with a REAL case to get the adrenaline pumpin’.
You are working a shift at your local level one trauma centre. You receive a pre-alert from EMS that they are coming in with a 45Y male with a significant neck wound. In an attempt to take his own life, the patient took a butcher knife and slashed his throat. The paramedic describes the wound as bleeding profusely and that when they looked at it, it was “like an anatomy prosection”. Your triage nurse looks at you and says “What are we gonna do?!” Your mind races trying to remember the zones of the neck, airway considerations, imaging specifics, and just as you start to make a plan, the patient rolls through the door.
If this case fills you with dread, fear not. Today’s episode reviews all of the relevant materials contained within Chapter 37 in Rosen’s 9th Edition. We will break down the anatomy, outline relevant imaging and management decision points, and give you some additional pearls to help you in the event that this case (or one like it) rolls through your ED doors on your neck shift. As always, we will pepper the episode with some classic exam fodder as per usual to make sure you got the skills to thrills on paper and in the trauma bay. So, sit back, grab a cup of coffee, and enjoy the ride!
[1] Outline the anatomic borders of the anterior and posterior triangles of the neck.
Bit of an easy one to start us off.
- The anterior triangle of the neck:
- Anterior = midline
- Posterior = sternocleidomastoid muscle
- Superior = lower edge of the mandible
- The posterior triangle of the neck:
- Anterior = sternocleidomastoid muscle
- Posterior = trapezius muscle
- Inferior = clavicle
Note: The anterior triangle is PACKED FULL of important structures, making an injury to this area far less favorable than to the posterior triangle
[2] Detail the borders and associated contents of the three zones of the neck. (Box 37.1)
Ahhhh, the zones of the neck – a classic question with questionable significance. Prior to the advent of modern imaging technologies, the zones of the neck had real implications for ED clinicians and surgeons alike. However, now that CT/CTA has become commonplace and the literature demonstrates that most significant penetrating neck injuries damage more than one zone , this classification system has fallen by the wayside in some centers. Despite this, we will review it here.
Zone I – base of the neck – extends superiorly from the sternal notch and clavicles to the cricoid cartilage
Zone II – midneck – extends from the cricoid cartilage to the angle of the mandible
Zone III – upper neck – extends from the angle of the mandible to the base of the skull
The following table is adapted from Box 37.1 – Vascular and Other Contents in Neck Zones, from Rosen’s 9th Edition. Please refer to the text for further clarification.
| Vascular and Other Contents in Neck Zones |
| Zone I |
| Proximal common carotid artery Vertebral artery Subclavian artery Major vessels of the mediastinum Apices of the lungs Esophagus Trachea Thyroid Thoracic duct Spinal cord |
| Zone II |
| Carotid artery Vertebral artery Larynx Trachea Esophagus Pharynx Jugular Vein Vagus nerve Recurrent laryngeal nerve Spinal cord |
| Zone III |
| Distal carotid artery Vertebral artery Distal jugular vein Salivary and parotid glands Cranial nerves IX-XII Spinal cord |
[3] List 5 hard and 5 soft signs of penetrating neck trauma (Box 37.2)
The following table is adapted from Box 37.2 – “Soft” and “Hard” Signs of Penetrating Neck Trauma from Rosen’s 9th Edition. Please refer to the text for further clarification.
| “Soft” and “Hard” Signs of Penetrating Neck Trauma |
| Hard Signs |
| Rapidly expanding/pulsatile hematoma Massive hemoptysis Air bubbling from wound Severe hemorrhage Shock not responding to fluids Decreased or absent radial pulse Vascular bruit or thrill Stridor/hoarseness or airway compromise Cerebral Ischemia +/-Massive subcutaneous emphysema |
| Soft Signs |
| Minor hemoptysis Hematemesis Dysphonia Dysphagia Subcutaneous or mediastinal free air Non Expanding hematoma Orotracheal bleeding Neurological findings Proximity wound |
In general, knowing the hard and soft signs will help with immediate patient disposition decisions. If any hard signs are present, the patient should undergo expedited transport to the OR (depending on institutional factors). Soft signs, if present, require further diagnostic evaluation. The initial imaging study most commonly ordered is a CTA of the neck +/- head, but further investigations depending on the suspected structures injured (e.g., esophagus) require other testing.
[4] List 5 hard and 5 soft signs of vascular injury
Given the similarities between the signs of penetrating neck and vascular injuries, we thought we’d give you a list here. It is important to form linkages between different lists in your brain before exam time, and this is the perfect example of where remembering one will help you remember much of the other.
| “Soft” and “Hard” Signs of Vascular Injury |
| Hard Signs |
| Rapidly expanding/pulsatile hematoma Arterial pulsatile bleeding Presence of bruit or thrill Obvious arterial occlusion as evidenced by: Pain Pulselessness Pallor Poikilothermia Paralysis Paresthesias |
| Soft Signs |
| History of significant or pulsatile bleeding at scene Proximity of penetrating wound or blunt trauma to major artery Diminished unilateral distal pulse Small non-pulsatile hematoma Peripheral nerve deficit Abnormal ankle-brachial index (<0.9) Unexplained hypotension High risk orthopedic injuries |
[5] Outline an approach to the management of a patient with a hemorrhaging penetrating neck wound.
Alright, so you have a patient with a hemorrhaging penetrating neck wound. Here is a stepwise approach to the management:
- Open wounds should first be covered and sufficient compression should be applied to stop bleeding and prevent the ever-dreaded air embolism. Avoid probing or blind clamping these injuries because MASSIVE BLEEDING and DAMAGE TO SURROUNDING STRUCTURES are things we like to avoid.
- Simultaneously have multiple sites of IV access placed on the side opposite the injury, avoiding the ipsilateral neck or upper extremity. Begin PRBC administration or massive transfusion protocols if appropriate.
- If significant and potentially life-threatening bleeding continues, insert your gloved fingers into the wound to directly tamponade the site.
- If this fails, pack the wound while maintaining pressure
- As a last resort, consider inserting a 16-18 French ballooned catheter into the wound and inflate. This may buy you time to transport to the operating theatre.
Unfortunately, these measures fail from time to time. This is particularly the case when sites of bleeding are in zones I and III of the neck, where direct tamponade is not possible.
[6] Describe the management of a patient with a suspected venous air embolism.
Venous air embolism is a condition in which a significant volume of air (50 mls or more) enters the venous system, circulating through the right heart and into the pulmonary circulation. Penetrating neck trauma is particularly high risk for the development of air emboli particularly because a negative venous pressure is created (blood flows down to the heart), and as a result, sucks air into the venous system.
Classically, patients who develop venous air embolism experience sudden-onset respiratory distress and develop rapid onset obstructive shock and hemodynamic collapse.
Here is a stepwise approach to the management of a suspected venous air embolism:
- Place the patient head down
- Position the patient in left lateral decubitus position, allowing the embolus to accumulate in the apex of the RV
- Aspirate air from the RV with US guided pericardiocentesis or under direct visualization after ED thoracotomy
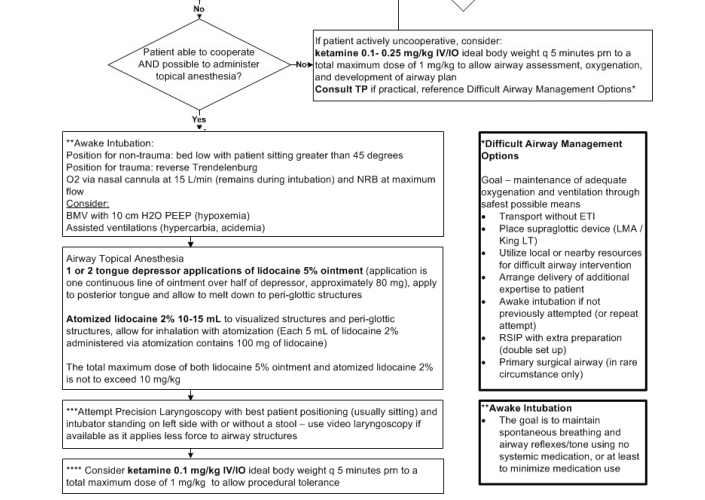
[7] Outline the steps in performing an awake intubation.
This is one of the most hotly debated topics in airway intervention literature. In general, the awake intubation is indicated when the patient has anatomic predictors of difficulty that would make RSI more difficult. The goal of performing an awake intubation is to maintain spontaneous breathing and airway reflexes to prevent decompensation and subsequent loss of the airway completely.
While airway management in the setting of neck trauma is complex and made difficult for a multitude of reasons in these patients, considering an awake intubation for these patients (if possible) is important. This procedure requires a significant amount of planning and the entire team must work in unison to get the job done.
The following is an algorithm from our friends at STARS (Shock Trauma Air Rescue Service) will help you to ace your next awake intubation.
[8] Outline the indications for imaging to screen for blunt cerebrovascular injury. (Table 37.2)
The dreaded blunt cerebrovascular injury is something clinicians have poorly identified for decades. There are multiple reasons for this, however, the bulk of the blame can be placed on one feature of this disease process: THE TIMING. Unfortunately, neurological symptoms of blunt CVI are often delayed, with the median onset being 12.5 hrs post-injury. What’s more, up to ⅓ of patients show no neurological deficit for more than 24 hours.
We have tried time and time again to create tools to help us find persons with asymptomatic CVI’s, but even now, many fall short. In fact, no single set of screening guidelines has been accepted because they are all too insensitive. For exam purposes, we have outlined the recommendations for screening from the Western Trauma Association and the Eastern Trauma Association. Be mindful that these may change in the coming years.
The following table is adapted from Table 37.2 – Trauma Association Criteria for Blunt Cerebrovascular Screening from Rosen’s 9th Edition. Please refer to the text for further clarification.
| Symptomatology | Western Trauma Association | Eastern Trauma Association |
| Symptomatic | Arterial hemorrhage from the neck, mouth, nose, ears Large or expanding cervical hematoma Cervical bruit in patients <50Y Focal neurological deficit Evidence of cerebral infarct Neurologic deficit incongruous with CT/MR findings | Unexplained neurological injury Arterial epistaxis |
| Asymptomatic | Cervical hyperextension or hyperflexion with rotation as mechanism Direct cervical trauma Intraoral trauma Basilar skull fracture involving the carotid canal LeFort II or III Head injury with GCS <6 Fracture of C1-C3 Vertebral body or transverse foramen fracture, subluxation, or ligamentous injury at any level Hanging with cerebral anoxia Seatbelt sign or clothesline injury with significant cervical pain, swelling, AMS | GCS <9 Petrous bone fracture DAI Cervical spine fracture (especially C1-C3, transverse foramen, or subluxation/rotational component) LeFort II or III fracture |
[9] Detail the appropriate imaging studies to order in the patient at risk for or with suspected blunt cerebrovascular injury.
So, we all know these patients are getting the good ol’ CTA neck +/- head. This has become standard. But, what if, despite negative CTA, the patient still has symptoms suggestive of a blunt CVI? Well, let’s talk numbers.
CTA for blunt CVI is actually not as good as everyone thinks it is. It’s sensitivity for these injuries is approximately 51%. And of those lesions missed by CTA, 80% are pretty serious (ie., grade 2 or higher). CTA also frequently produces false positives in the context of blunt neck trauma. In comparison, the tried and true digital subtraction angiography (DSA) has a sensitivity of 89-100%. It has a complication rate of <2%.
So, how should we go about looking for a blunt CVI? Well, it all depends on pretest probability. If you have a high pretest probability for this injury, you cannot stop at a CTA. If the CTA is negative, get the DSA.
Wisecracks:
[1] What structure, if violated, should make you suspect injury to the deep tissues of the neck?
Answer:
The platysma muscle. If this structure is violated, injury to deep structures SHOULD BE SUSPECTED.
[2] What study or studies is/are indicated to evaluate a patient for suspected esophageal injury.
Answer:
- Contrast esophagography (typically with gastrografin); can use barium, but there exists an increased danger from extravasation.
- Flexible endoscopy
This is important, as the vast majority of these patients will get a CTA neck +/- head for investigations. While a very good test for the sequelae of penetrating neck injuries, the sensitivity of this test is variable for esophageal injuries, being quoted in Rosen’s as being as low as 50% . The sensitivity does increase when paired with a contrast swallowing study. However, if you want a sensitivity approaching 100%, get the contrast swallowing study followed by flexible endoscopy.
[3] List 4 mechanisms of morbidity and mortality that occur as the result of vascular injury in the neck.
Answer:
- Exsanguination
- Hematoma expansion with subsequent airway distortion and compromise
- Direct vessel injury leading to vascular occlusion
- Embolization of a foreign body
[4] What is the most common mechanism of injury causing blunt cerebrovascular injury?
Answer:
As per Rosen’s 9th Edition, the most common mechanism causing blunt internal carotid injury is sudden forceful hyperextension with lateral rotation of the neck
[5] List 3 mechanisms that cause pulmonary edema in a patient post-hanging.
Answer:
- Postobstructive pulmonary edema (similar to negative pressure pulmonary edema in the Anesthesiology literature)
- Neurogenic pulmonary edema
- Cardiogenic pulmonary edema secondary to pathologies like Takotsubo cardiomyopathy
[bg_faq_end]
This post was copyedited by Dillan Radomske (Twitter: @DillanRadomske)

Dillan Radomske
Latest posts by Dillan Radomske (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021

Owen Scheirer
Latest posts by Owen Scheirer (see all)
- CRACKCast E231- Genitourinary System - April 1, 2022
- CRACKCast E228 – Neck Trauma - August 6, 2021
- CRACKCast E226 – Facial Trauma - June 10, 2021