
This updated episode of CRACKCast covers Rosen’s Chapter 36 (9th Ed.) on spinal injuries. This episode will outline the approach and details of the diagnosis, classification and treatment of spinal trauma in the emergency department.
Shownotes – PDF Here
[bg_faq_start]Rosen’s in Perspective
Alright, podcast listeners. We are back at it again with another episode of CRACKCast. Today, we will be reviewing Chapter 36 – Spinal Injuries in Rosen’s 9th Edition. This is one of the lengthy chapters in the Bible of EM, so make sure to allot time to crush out the chapter readings.
Anyone who has worked in the ED for any significant period of time will know how debilitating spinal injuries can be. We have all seen our fair share of complex traumas and are relatively comfortable with the initial management strategies for these injuries. However, what many of us fail to recognize is the true significance of these injuries. As is the case with many of the disease processes we manage every day, the effects of spinal cord injuries extend far beyond the resuscitation bay. Often, patients who sustain significant trauma suffer lifelong physical, psychiatric, and socioeconomic issues as a result. It is estimated that the lifetime cost of care for paraplegic SCI victims in the US ranges from $ 1 million in those older than 50 to $4 million for those younger than 25. Moreover, the total societal cost is far more, costing $5 billion in lifelong medical expenses and lost productivity for all ages and types of SCI’s. Thus, it is paramount that ED clinicians know how to assess for, treat, and refer these patients appropriately.
If you feel like you could use a refresher on the topic, please listen up. Today, we will review some of the relevant content you will need to know on your next shift in the thunderdome. So, as always, grab a cup of coffee, take a deep breath, and enjoy the show!
[bg_faq_end]Core Questions:
[bg_faq_start][1] Outline the Denis Classification system for determining the stability of spinal injuries
- The Denis Classification is a model that divides the spine into 3 parallel vertical columns
- Anterior – formed by the alternating vertebral bodies and intervertebral disks surrounded by the annulus fibrosus (capsule) and anterior longitudinal ligament
- Middle – formed by the posterior portion of the annulus fibrosis and posterior vertebral wall, posterior longitudinal ligament, spinal cord, paired laminae and pedicles, articulating facets, transverse process, nerve roots, and vertebral arteries and veins
- Posterior – formed by the spinous processes, nuchal ligament, interspinous ligament, supraspinous ligament, and ligamentum flavum
- Typically, this model allows for a single column to be affected by an injury without causing instability.
- Disruption of two columns results in an injury that is stable in one direction but unstable in another.
- Disruption of all three columns results in a HIGHLY MULTIDIRECTIONAL UNSTABLE INJURY

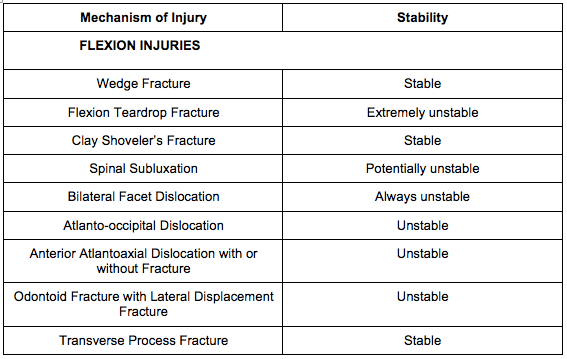
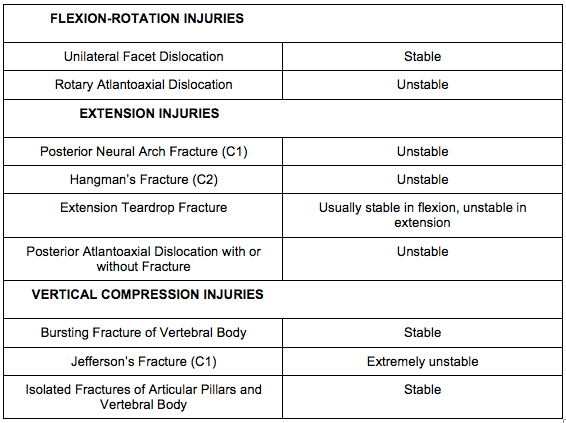
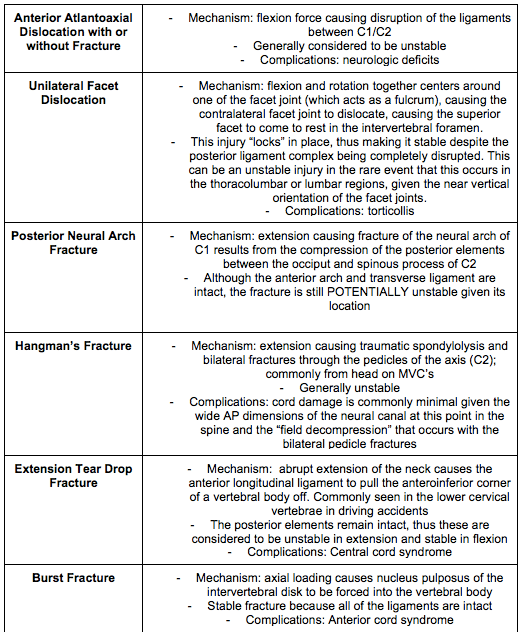
[2] List 5 flexion, 2 flexion-rotation, 3 extension, and 2 vertical compression spinal injuries (Table 36.1)
The following table is modelled after Table 36.1 – Classification of Spinal Injuries in Rosen’s 9th Edition. Please refer to the text for further clarification.
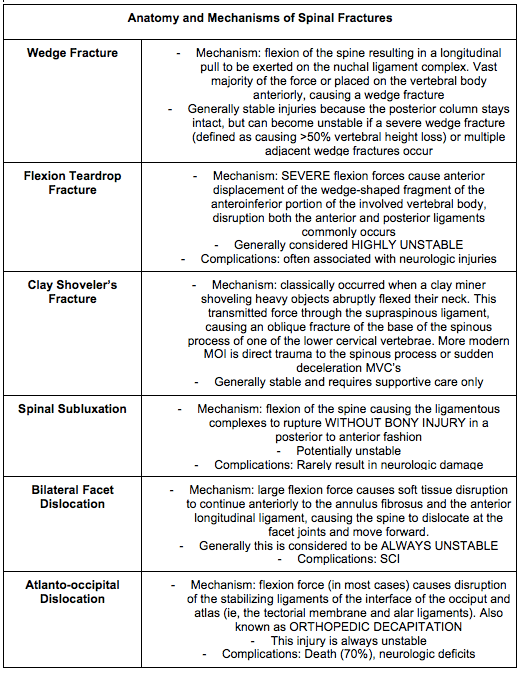
[3] Outline the mechanisms and potential complications of the following flexion injuries:
[4] How are odontoid fractures classified and what causes them?
- Odontoid fractures are typically caused by trauma to the head in the anteroposterior direction.
- Odontoid fractures are typically classified into three categories:
- Type I – fracture to the odontoid ABOVE the transverse ligaments; typically stable as they are only an avulsion fracture to the tip of the odontoid, but becomes unstable if there is damage to the apical and alar ligaments
- Type II – fracture to the odontoid at the base where it attaches to C2 – unstable, often complicated by non-union
- Type III – fracture to the odontoid at the base where it attaches to C2 WITH EXTENSION INTO the body of C2 – unstable, can extend laterally into the superior articular facet of the atlas
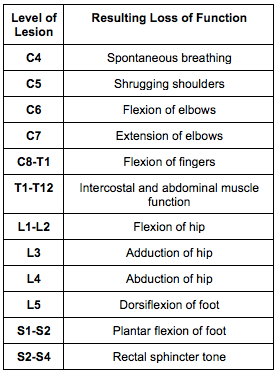
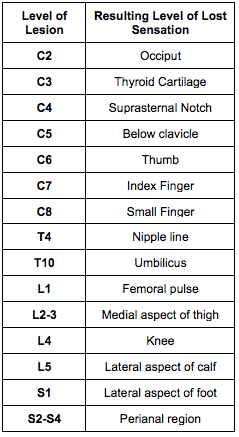
[5] Organize the spinal motor, sensory, and reflex examinations based on spinal levels. (Tables 36.3, 36.4, 36.5)
This table has been adapted from Table 36.3 in Rosen’s 9th Edition – Spinal Motor Examination. Please refer to the text for further clarification.
This table has been adapted from Table 36.4 in Rosen’s 9th Edition – Spinal Reflex Examination. Please refer to the text for further clarification.

This table has been adapted from Table 36.5 in Rosen’s 9th Edition – Spinal Sensory Examination. Please refer to the text for further clarification.
[6] Detail the following cord syndromes:

[7] List the components of the following imaging decision-making tools: Canadian C-Spine Rule, NEXUS C-Spine Rule.
Canadian C-Spine Rule

- Exclusion Criteria include:
- Age <16Y
- GCS <15
- Grossly abnormal vital signs
- Injury >48 hrs old
- Penetrating trauma
- Acute paralysis
- Known vertebral disease (ankylosing spondylitis, rheumatoid arthritis, spinal stenosis, previous spinal surgery)
- Return visit for reassessment of same injury
- Pregnant
NEXUS C-Spine Rule:
- No midline tenderness
- No focal neurological deficit
- No abnormal alertness
- No intoxication
- No painful distracting injury
If all criteria are met, no C-spine imaging is required.
[bg_faq_end]Wisecracks:
[bg_faq_start][1] How do you calculate Power’s Ratio and why is it important?
Answer:
- Power’s Ratio is calculated in the following manner:
- First, measure the distance between the basion and the mid vertical portion of the posterior laminar line of the atlas (commonly referred to as BC)
- Then, measure the distance between the opisthion to the mid vertical portion of the posterior surface of the anterior ring of the atlas (commonly referred to as OA)
- After, divide BC by OA to get the ratio
- A value of > 1 indicates subluxation of the atlas and axis
- THESE ARE UNSTABLE INJURIES because of the paucity of muscle and ligamentous support in this area of the spine
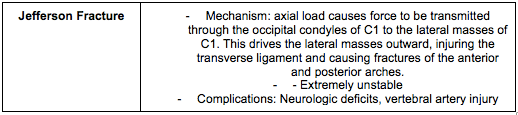
[2] What injuries is the open-mouth odontoid radiograph best at visualizing?
Answer:
- Dens Fracture
- Jefferson’s Fracture
- Transverse Ligament Injury
- Basilar Invagination
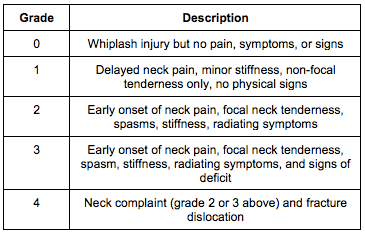
[3] How are whiplash-associated injuries classified?
Answer:
This table has been adapted from Table 36.2 in Rosen’s 9th Edition – Quebec Task Force Classification of Whiplash-Associated Disorders. Please refer to the text for further clarification.
[4] At what spinal level would you expect an injury to potentially cause Horner’s Syndrome?
Answer:
- Horner’s Syndrome, characterized by unilateral ptosis, miosis, and anhidrosis results from disruption of the cervical sympathetic chain
- Thus, injuries occurring between C7 and T2 could produce Horner’s Syndrome
[5] What is spinal shock and what physical exam finding indicates its end?
Answer:
As per Rosen’s 9th Edition: “Spinal shock results from a concussive injury to the spinal cord that causes total neurologic dysfunction distal to the site of injury. The end of spinal shock is heralded by the return of the bulbocavernosus reflex.”
[bg_faq_end]Shownotes copyedited and uploaded by Ryan Fyfe-Brown

Ryan Fyfe-Brown
Latest posts by Ryan Fyfe-Brown (see all)
- CRACKCast E227 – Spinal Injuries - July 16, 2021