

This episode of CRACKCast covers Rosen’s Chapter 105, Brain and Cranial Nerve Disorders. These can be the weird and wonderful in the ED, but subtle hints can clue us in that further investigation is needed for our patients. Having a high suspicion for these diagnoses can help you make an appropriate care plan and follow up for patients with neurological disease.
Shownotes – PDF Here
[bg_faq_start]Rosen’s in Perspective
What are three things I can guarantee you feel a little queasy when pimped about? Well we’ve got you covered here for Cranial Nerve problems, Cerebral Venous Thrombosis and Multiple Sclerosis. When it comes to Cranial nerve deficits, remember to NOT MISS THE INTRACRANIAL CATASTROPHE! When deficits cannot be clearly attributed to lower motor neuron dysfunction, obtain definitive imaging (typically, a CT head +/- contrast or MRI).
Why do we give anti-virals to treat viral neuropathy?
Answer: From UptoDate
- Lessen the severity and duration of pain associated with acute neuritis
- Promote more rapid healing of skin lesions
- Prevent new lesion formation
- Decrease viral shedding to reduce the risk of transmission
- Prevent PHN
[1] List the name, function and pathologic features of the cranial nerves
Refer to figure 95.1 in Rosen’s 9th Edition for a more comprehensive table summarizing cranial nerve function and pathologic features when injured
| Cranial Nerve | Function of Nerve | Presentation |
| CN I: Olfactory N. | Gustatory sense | Unilateral anosmia |
| CN II: Optic N. | Sight | Unilateral vision loss |
| CN III: Oculomotor N. | Motor function of levator palpebrae, superior rectus, medial rectus, inferior rectus, and inferior oblique muscles; pupillary constriction | Ptosis, eye deviated laterally and downward, diplopia, dilated and non-reactive pupil, loss of accommodation |
| CN IV: Trochlear N. | Motor function of superior oblique | Inability to move eye downward and laterally, diplopia, head tilt toward unaffected eye |
| CN V: Trigeminal N. | Sensation of face, scalp, and oral cavity; motor function of masseter and temporalis muscles/tensor tympani | Partial facial anesthesia, periodic lancinating facial pain |
| CN VI: Abducens | Motor function of lateral rectus muscle | Diplopia, inability to move affected eye laterally |
| CN VII: Facial N. | Motor function of muscles of facial expression; PSNS innervation of lacrimal and salivary glands; sensation of ear canal and tympanic membrane | Hemifacial paresis, abnormal taste, sensory deficit around ear, sensitivity to loud sounds |
| CN VIII: Vestibular N. | Hearing and balance | Vertigo, tinnitus, unilateral hearing loss |
| CN IX: Glossopharyngeal N. | Taste and sensation of posterior aspect of tongue, motor function of stylopharyngeus | (RARE) Intermittent pain in the pharynx |
| CN X: Vagus N. | Motor function of smooth and striated muscles and glands of the pharynx, larynx, and veli palatini; motor function of smooth muscle of the thoracic and abdominal viscera; sensory input from the pharynx, larynx, esophagus, and thoracic/abdominal viscera | Loss of palate rise, dysphagia, hoarse voice |
| CN XI: Spinal Accessory N. | Motor function of the sternocleidomastoids and trapezius muscles | Shoulder drop and downward displacement of scapula |
| CN XII: Hypogossal N. | Motor function of tongue | Tongue deviations |
[2] List 6 differential diagnoses for facial pain / trigeminal neuralgia
Here is the list from Rosen’s:
- Odontogenic infections
- Sinus disease
- Otitis media
- Acute glaucoma
- Temporomandibular joint disease
- Herpes zoster
Note: However, you need to remember the basics here. Craniofacial pain can come from sensory fibres from any of the following nerves. So, any disease entity involving any combination of the listed nerves needs to be considered:
- Trigeminal (CN V)
- Nervus intermedius (CN VII)
- Glossopharyngeal (CN IX)
- Vagus (CN X)
- Upper cervical spinal cord roots
[3] Trigeminal neuralgia – describe the diagnosis and management
Note: Trigeminal neuralgia = tic douloureux
Symptomatology: idiopathic pain in one or more distributions of the trigeminal nerve (CN V). The vast majority of cases (90%) result from vascular compression of the trigeminal nerve root
RF:
- Female-to-male ratio of 2:1
- 50 – 69 years old
- Right side of the face > Left side
Diagnosis: Clinical Syndrome
- Normal head and neck examination
- No neurologic deficits
- Episodic, unilateral facial pain associated with non-painful triggers
Management:
Mainstay = Carbamazapine 100mg PO BID.
Other options:
- Phenytoin
- Baclofen
- Valproate sodium
- Lamotrigine
- Gabapentin
- Levetiracetam
Disposition: Neurology with +/- Neurosurgery or ENT consult if surgical decompression is required
[4] Facial nerve paralysis: List 6 differential diagnoses for facial (CN VII) paralysis
- Bell’s palsy
- Ramsey Hunt syndrome (herpes zoster oticus)
- Lyme disease (neuroborreliosis)
- Bacterial infections of the middle ear, mastoid, or external auditory canal
- Guillain-Barré syndrome
- HIV infection
- Tumor compressing nerve (from temporal bone, internal acoustic canal, cerebellopontine angle, or parotid gland)
- Stroke (rare) (the rare pons stroke can mimic LMN facial nerve palsy)
- Sjögren’s syndrome (rare)
- Sarcoidosis (rare)
- Melkersson-Rosenthal syndrome (rare): “condition with a female predominance characterized by recurrent episodes of facial paralysis, episodic facial swelling, and a fissured tongue” – UptoDate
[5] Describe the facial weakness deficit associated with Bell’s Palsy and list 3 other associated symptoms
- Sudden onset (think hours) unilateral facial paralysis
- Eyebrow sagging
- Inability to close the eye
- Disappearance of the nasolabial fold
- Drooping at the affected corner of the mouth, which is drawn to the unaffected side
- Decreased tearing
- Hyperacusis
- Loss of taste sensation on the anterior two-thirds of the tongue
Note: There is a way to classify the nerve dysfunction
| House-Brackmann classification of facial nerve dysfunction | |
| Grade | Finding |
| I | Normal |
| II | Mild dysfunction |
| III | Moderate dysfunction |
| IV | Moderately severe dysfunction |
| V | Severe dysfunction |
| VI | Total paralysis |
[6] List 4 components of treatment of Bell’s Palsy, and list the symptoms that would make you suspect Lyme Disease
- Glucocorticoids
- Antivirals for severe disease (controversial with poor evidence but recommended for Grade IV and higher)
- Eye care (artificial tears)
- Physiotherapy (controversial)
See Table 95.2 in Rosen’s 9th Edition for dosing of steroids and antivirals in Bell’s Palsy
Consider Lyme (or infectious mononucleosis) disease if:
- Systemic symptoms
- Bilateral facial paresis
Remember: caused by the spirochete Borrelia burgdorferi from Ixodes genus ticks
[7] Differentiate between herpes zoster ophthalmicus and herpes zoster oticus
Herpes zoster ophthalmicus = shingles of the trigeminal nerve
- Hutchinson’s sign: cutaneous involvement of nasociliary nerve
- Look for ocular involvement = punctate epithelial erosions and pseudodendrites
Herpes zoster oticus = Ramsay Hunt syndrome
- Unilateral facial paralysis
- Can precede rash by days
- Herpetiform vesicular eruption
- Pinna, external auditory canal, tympanic membrane, soft palate, oral cavity, face, and neck as far down as the shoulder
- Vestibulocochlear dysfunction
[8] Describe the symptoms and diagnostic test for vestibular schwannoma
Note: vestibular schwannoma = acoustic neuroma
Symptomatology: patients with sudden sensorineural hearing loss
Diagnosis: ENT referral and MRI with gadolinium
[9] What is the pathophysiology of diabetic mononeuropathy and which nerves are usually involved?
Note: Diabetics are at high risk of intracranial badness!!! Look for brainstem pathology
Diagnosis: DIAGNOSIS OF EXCLUSION
Symptomatology: Think about in diabetics with oculomotor nerve (CN III) palsy with sparing of the pupillary response
[10] What is Uhthoff’s phenomenon?
*** Elevated body temp = worsening demyelinating disease symptoms ***
Definition: “Uhthoff’s phenomenon (also known as Uhthoff’s syndrome, Uhthoff’s sign, and Uhthoff’s symptom) is the worsening of neurologic symptoms in multiple sclerosis (MS) and other neurological, demyelinating conditions when the body gets overheated from hot weather, exercise, fever, or saunas and hot tubs. It is possibly due to the effect of increased temperature on nerve conduction. With an increased body temperature, nerve impulses are either blocked or slowed down in a damaged nerve but once the body temperature is normalized, signs and symptoms may disappear or improve.”
[11] List 10 clinical symptoms of MS, describe its diagnosis, and describe the typical CSF findings in a patient with MS
Note: Multiple sclerosis should be suspected in patients who present with episodes of neurologic dysfunction that evolve over days and resolve over weeks. Apparent exacerbations of known MS can be brought on by other medical problems, most commonly infections.
Diagnosis: The diagnosis of MS is accomplished using the McDonald Criteria. In summary, the patient must demonstrate disseminated central nervous system lesions over both space and time. This can be done based on either clinical findings alone or a combination of radiologic findings (use MRI) and clinical evidence of disease.
Symptomatology:
- Symptoms that suggest MS:
- Relapsing and remitting symptoms
- Onset between 15-50 years of age
- Optic neuritis
- Lhermitte’s sign (electric shock sensations that radiate down back/limbs with flexion of the neck)
- Intranuclear opthalmoplegia
- Fatigue
- Uhthoff’s phenomenon
- Typical MS Symptoms:
- Sensory disturbances in limbs
- Vision loss
- Motor disturbances
- Diplopia
- Gait disturbance
- Imbalance
- Sensory disturbances in face
- Lhermitte’s sign
- Vertigo
- Bladder issues
- Limb ataxia
- Acute transverse myelopathy
- Pain
CSF:
- CSF analysis is abnormal in 90% of the cases
- 50% patients have pleocytosis
- More than 5 lymphocytes /HPF
- ~70% of patients have increased immunoglobulin G (IgG) ranging from 10% to 30%
- Increased oligoclonal bands of IgG in 85% to 95% (oligo bands are also seen in neurosyphilis, fungal meningitis, and other CNS infections)
[12] What is the management of an acute MS exacerbation and what is the usual management of a patient with relapsing-remitting MS who presents with a flare?
- Consult their primary neurologist!
- IV methylprednisolone, 250 to 500 mg every 12 hours for 3 to 7 days effectively promotes earlier resolution of recurrences.
- IV methylprednisolone has been shown to speed the recovery from vision loss from optic neuritis associated with MS.
Relapsing remitting:
- Initiate treatment with interferon-β or glatiramer acetate.
- Newer disease-modifying agents include a bunch of -MABs: laquinimod, daclizumab, natalizumab, and terifunomide
- Facial pain: Carbamazapine
- Tremor: Propranolol or Benzos
- Spasticity: Baclofen
Wise Cracks:
[1] Cerebral Venous Thrombosis Bounceback: What are the key pearls?
Four risk factors for cerebral venous thrombosis:
- Transient risk factors
- Infection – think any HEENT or systemic infection
- Pregnancy
- Dehydration
- Head injury / trauma / post-neurosurgery
- Drugs:
- OCPs, HRT, androgens, tamoxifen, glucocorticoids
- Permanent risk factors
- Inflammatory disease: SLE, Behçet’s disease, GPanG, IBD, sarcoidosis
- Malignancy
- Hematologic conditions
- Procoagulant disease
- Antithrombin deficiency
- Protein C/S deficiency
- Factor V Leiden mutation
- Hyperhomocysteinemia
- Polycythemia
- Procoagulant disease
- Congenital heart disease
- Thyroid disease
What CT findings may be seen in cerebral venous thrombosis? What is the most common CT finding?
- Delta Sign / Dense Triangle / Empty Triangle Sign Ref: here

- Cerebral Edema
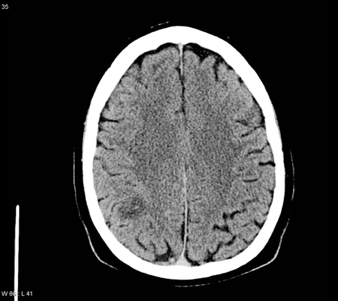
- Absent Venous Flow
- Hemorrhage secondary to venous congestion Ref: here
 =
=Pearls:
- ***Non–contrast-enhanced CT scanning is not adequate to rule out CVT***
- *** MRI with MRV is recommended***
- Treatment = systemic anticoagulation, even in the setting of hemorrhagic cerebral infarcts, unless another contraindication exists!!!
- Hemorrhage secondary to venous congestion Ref: here
[2] Which CN is most commonly injured in trauma?
*** Trigeminal Nerve: anesthesia dolorosa ***
Definition: According to UptoDate:“Painful post-traumatic trigeminal neuropathy (anesthesia dolorosa) — Painful post-traumatic trigeminal neuropathy, also known as anesthesia dolorosa, is characterized by unilateral facial or oral pain that occurs after traumatic injury of the trigeminal nerve, accompanied by additional symptoms or signs of trigeminal nerve dysfunction. This condition is a perfect example of how difficult central pain can be to describe since the patient has sensory loss, but at the same time, can feel pain. In anesthesia dolorosa, pain is superimposed in an area of the face that either lacks or has impaired sensation.”
[3] What syndrome is associated with bilateral acoustic neuromas?
Approximately 5% of cases and generally associated with Type 2 Neurobromatosis
[4] How is diabetic mononeuropathy treated?
NO CURE. Improve glucose control. Resolution within 3-6months.Treatment consists of:
- Patching the affected eye
- Administration of analgesics
- Antiplatelet therapy
This post was uploaded and copyedited by Riley Golby (@RileyJGolby)
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018

Adam Thomas
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018