

This episode of CRACKCast covers Rosen’s Chapter 18, Seizures. This topic covers the basics of seizures, and the management of status epilepticus.
PDF Show Notes – Link Here
[bg_faq_start]Rosen’s in Perspective:
- seizures are a pathologic excess of neuronal activity that disrupt normal cortical or deep limbic system functioning
- the term epilepsy refers specifically to recurrent unprovoked seizure activity from genetic or acquired brain disorder
- general prevalence of epilepsy is 3% in population
- 10% of population will have a seizure at some point
Seizure categorization:
1) Cause: Primary or Secondary (provoked)
2) Effect on mentation: Generalized (tonic-clonic, absence, atonic, myoclonic) or focal
3) Motor activity: convulsive or non-convulsive
There are 6 factors that define an ictal event:
1. abrupt onset
2. brief duration
3. loss of consciousness
4. purposeless activity
5. unprovoked
6. postictal state
Was the incident truly a seizure?
Seizure characteristics
| Abrupt onset | generalized seizure usually occur without aura |
| Brief duration | rarely last longer than 10-20 seconds (usually over-estimated by bystanders) |
| Loss of consciousness | present, unless it is a focal seizure |
| Purposeless activity | automatisms, undirected tnic-clonic movements |
| Unprovoked | not provoked by emotional stimuli(exceptions: fever in children and substance withdrawl in adults |
| Post-ictal state | acute altered state occurs post-seizure (except focal or absence seizures) |
Simple febrile seizure most common pediatric seizure. Age 6 months to 5 years. Prevalence is 2-5%. 30% of these patients have 1 recurrence.
Red flag: febrile seizure in <6 months, prolonged seizure in any age group, or focal seizure[bg_faq_end]
[bg_faq_start]
1) What defines status epilepticus?
Various definitions:
Old definition: at least 30 min of seizure activity – changed because the longer somebody seizes the worst their outcome
New definition: 5 or more minutes of persistent seizures OR a series of recurrent seizures without return to FULL consciousness in between[bg_faq_end]
[bg_faq_start]
2) List the doses of common medications used for status epilepticus
First line agents:
Benzodiazepines
- Diazepam – 0.15 mg/kg IV
- can be given rectally
- Lorazepam – 0.1 mg/kg IV
- preferred IV agent: longer half-life
- Midazolam – 0.2 mg/kg IV / IM / IN
- preferred for IM or buccal
All effective. Give two max doses of benzos then switch to second line.
If multiple doses are needed and patient desaturates → intubate avoid long term neuromuscular blockade if possible (rare case where sux. could be used – consider checking K+ on a blood glass) consider EEG for monitoring of epileptiform brain activity
Second-line agents:
All agents are consensus based:
- all need to be given over 10 mins or so!!!
- Phenytoin – 20 mg/kg IV infusion
- Fosphenytoin (prodrug) – 20 mg/kg IV infusion Less tendency to cause hypotension and dysrhythmias
- Phenobarbital – 20-30 mg/kg IV infusion
- Valproic Acid – 20-40 mg/kg
- Levetiracetam
- Lacosamide
- Propofol infusion
- Age considerations:
- Adults 10mg Midazolam x 2, or 4mg Lorazepam x 2
- Benzo → Benzo →pheny/fosphenyoin → Phenobarbital/Valproate/Propofol
- Children 0.2+0.2 then rule of 20
- B → B → Phenobarbital → pheny/fosphenyoin
- Adults 10mg Midazolam x 2, or 4mg Lorazepam x 2
Refractory status epilepticus: “ seizures persistently unresponsive to third-line agents”
Treatment:
- Anesthetic doses of:
- midazolam
- propofol
- isoflurane anesthesia
Need non-depolarizing NMB and continuous EEG monitoring
Note: Keppra and Ketamine are new kids on the block. Avoid propofol in young children, as incidence of mitochondrial dysfunction is higher in this population and the mitochondrial suppression of propofol is theoretically harmful.[bg_faq_end] [bg_faq_start]
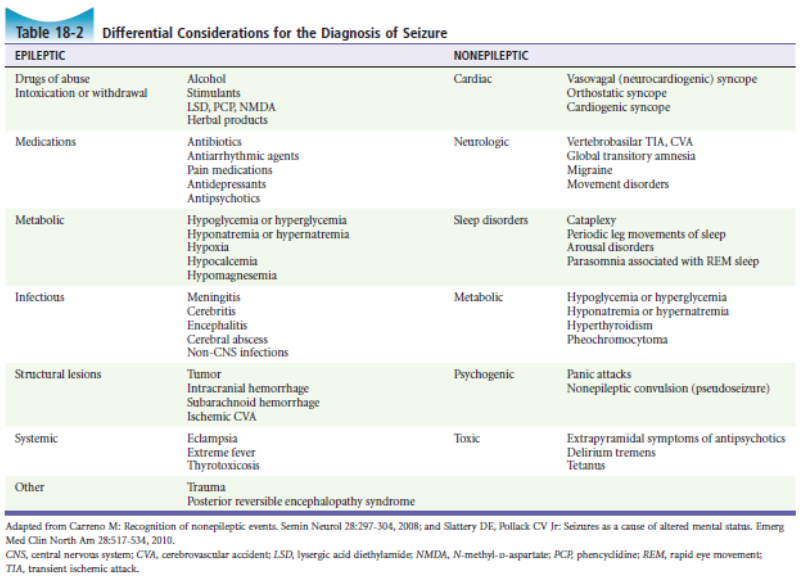
3) List 10 differential diagnoses for seizures
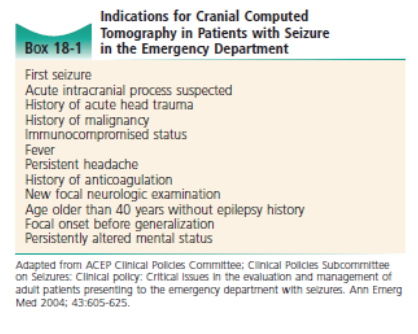
4) List 10 indications for head CT in new-onset seizure
Wisecracks:
1) How long does a driver in British Columbia require their driver’s license suspended after a seizure?
The Office of the Superintendent of Motor Vehicles publishes the BC Guide in Determining Fitness to Drive revised Jan 2016, See http://www2.gov.bc.ca/assets/gov/driving-andtransportation/driving/publications/factsheet-epilepsy.pdf.
Private drivers: 6 months seizure free
Professional drivers: 12 months seizure free
2) What are the special causes for seizure and their Tx?
Other aetiologies:
- hypoglucose
- give D10-25 for kids < 2 yrs (use the rule of 50s)
- can give D50 when > 2 yrs f.
- Isoniazid overdose: 0.5 g/min pyridoxine IV until seizure stops (max dose 70 mg/kg or 5 g)
- consider in prolonged refractory seizures despite benzo’s
- **pyridoxine is the only effective treatment**
- Eclampsia
- seizing woman of childbearing age –
- Consider in 20 weeks GA to up to 6 weeks postpartum
- Give IV magnesium 6 g over 15 mins h.
- seizing woman of childbearing age –
- Water intoxication / hyponatremia
- children, psych. patients, athletes
- treat with hypertonic saline
- 3% – 4-6 ml/kg over 1 hr (up to 100 ml)
- OR
- i) 5% hypertonic 50cc
- ii) 3% hypertonic 100ml-200ml over 1-2 hours iii)
- 6% Saline (2 amps bicarb)
- see: http://emcrit.org/pulmcrit/emergenttreatment-of-hyponatremia-or-elevated-icp-with-bicarb-ampules/ 3)
- treat with hypertonic saline
- children, psych. patients, athletes
3) What are the most common causes of status epilepticus?
As per table 18-1:
- antiepileptic drug associated – withdrawal or under dose ~ 25%
- ETOH related – 15-25%
- drug toxicity / post-stroke / CVA / metabolic (lytes) / hypoxia / post-arrest – 35%
- others: infection, cerebral tumour, trauma, idiopathic – 15%[bg_faq_end]
This post was edited and uploaded by Rob Carey (@_Robcarey)

Adam Thomas
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018