

This episode of CRACKCast covers Rosen’s Chapter 35, Back Pain. This chapter covers a diagnostic approach to a common ED complaint, with emphasis on the red flags you cannot miss, as well as an approach to treatment.
Shownotes – PDF Here
[bg_faq_start]1) List 10 historical red flags for back pain
Red flags on History and Physical Exam
- History
- Fracture risks:
- Trauma history
- Prolonged steroid use
- Frail, old, osteoporotic, over 70 years with or without MINOR trauma
- Smoking guns (historical)
- Syncope
- Children
- Acute onset with flank, testicular, or abdominal/back pain
- Diaphoresis
- Neurological deficits
- Cancer risks:
- Cancer history, weight loss, constitutional symptoms
- Worse at night or at REST
- Infection risks
- Immunocompromised, IVDU
- FEVER
- Fracture risks:
- Physical exam
- Vitals
- Hypo or hypertension, tachycardia, fever
- Unequal blood pressures in extremities
- Stethoscope
- Aortic insufficiency murmur – diastolic
- Palpation
- Circulatory compromise in lower extremities or pulse deficits
- Pulsatile abdominal mass
- Focal bony tenderness
- Neurological exam
- Urinary retention
- Loss of rectal sphincter tone (incontinence)
- Focal lower extremity weakness
- Vitals

2) List 6 emergent causes of back pain
See box 35-1 in Rosen’s (listed below)
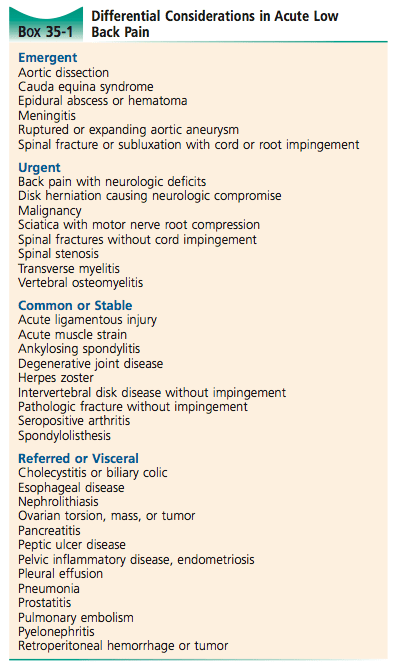
Emergent causes of back pain:
- Aortic dissection
- Cauda equina syndrome
- Epidural abscess / HEMATOMA
- Meningitis
- Ruptured or expanding abdominal aortic aneurysm
- Spinal fracture with subluxation causing CORD or ROOT impingement
Wisecracks
[bg_faq_start]1) Describe the most common sites of disc protrusion with their associated neurologic findings
Disc Protrusion and Signs:
Pathophysiology
- Systems involved:
- Vascular
- Visceral
- Infectious
- Mechanical
- Rheumatologic
- Anatomy to think through: spinal column, cord, root, muscles,
- Spinal cord ends at L1
Disc herniation
Normally the nucleus pulposus (gelatinous) is enclosed by the annulus fibrosus. With aging the annulus thins posteriorly which can lead to HERNIATION.
- Protrusion — extrusion — sequestration
- 95% of herniation occur at L4-S1 spaces – with associated radicular symptoms
- L5: decreased sensation to first webspace in foot
- Weak extension of the great toe and NORMAL reflexes
- S1
- Decreased sensation to lateral foot and small toe
- Weak plantar flexion and +/- ankle jerk reflex loss
- Disk extrusion – is usually symptomatic, the others usually are NOT
- L5: decreased sensation to first webspace in foot
- ⅔ resolve in 6 months on MRI
- 75% of people’s symptoms improve in 6 weeks
- If spinal stenosis, it worsens over time
- Imaging is NOT indicated unless cauda equina suspected / other risks / long course
- Compression above L1 = UMN findings
- Compression below L1 = LMN findings
2) Outline your approach to acute undifferentiated back pain
3) Describe your treatment approach for acute musculoskeletal low back pain
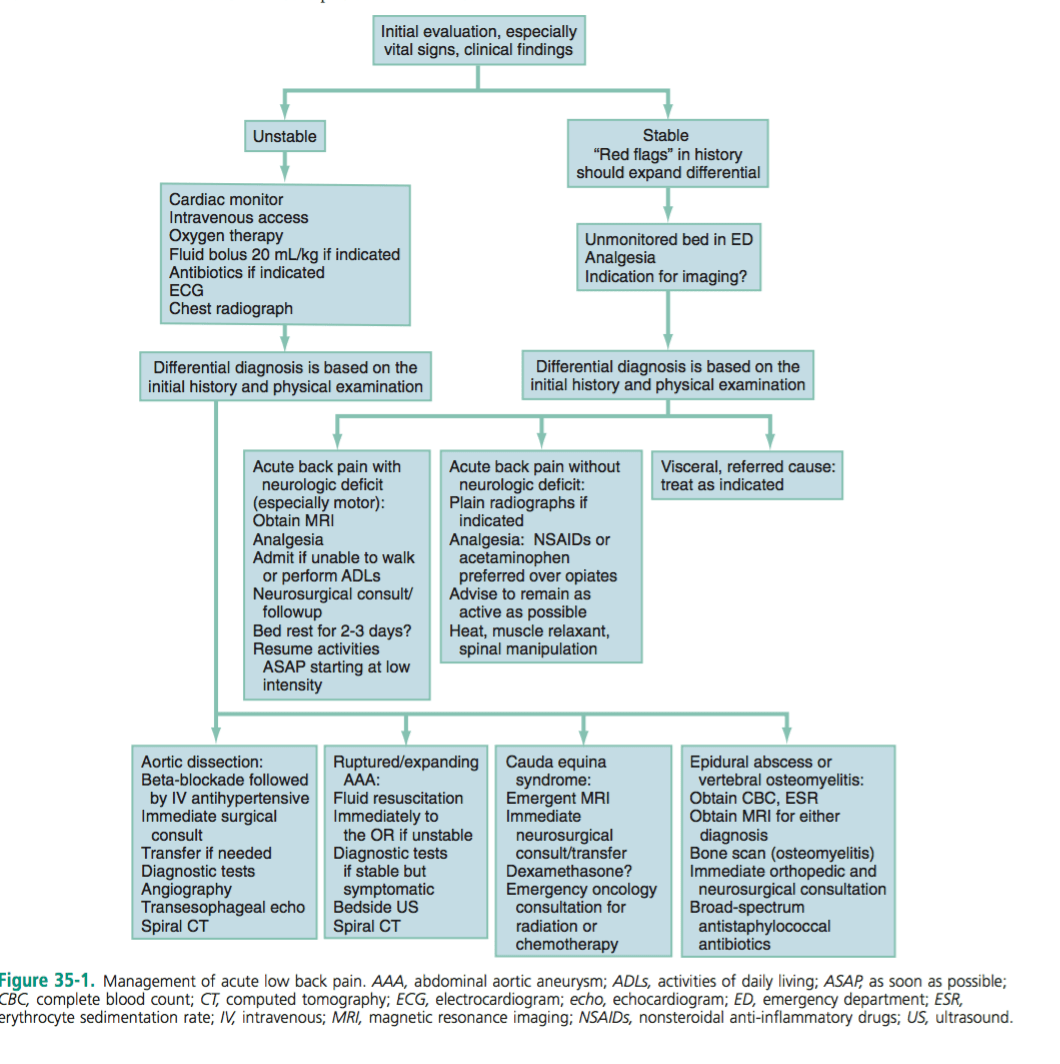
Empirical management
- Depends on presenting vitals signs and degree of illness – see fig 35-2
- If unstable: based on fig 35-1
- If stable:
- Severe pain:
- IV narcotics
- With transition to PO narcotics
- Moderate pain
- Tylenol and advil
- NSAIDS are NOT superior to tylenol and risks must be considered (patient factors!)
- IV narcotics
- Severe pain:
- Benzo’s:
- “Anxiolytic and sedative properties may promote sleep and synergize pain relief…”
- But dangerous
- Muscle relaxants:
- NO credible evidence supporting muscle relaxants or antispasmodic agents
- Methocarbamol or cyclobenzaprine
- Heat, spinal therapy, acupuncture, TENS
- Other therapies through family doctor:
- Gabapentin, TCAs, injections
- NEED a multidisciplinary approach to acute on chronic spells of back pain!
- NO credible evidence supporting muscle relaxants or antispasmodic agents
This post was uploaded and copyedited by Colin Sedgwick (@colin_sedgwick)

Adam Thomas
CRACKCast Co-founder and newly minted FRCPC emergency physician from the University of British Columbia. Currently spending his days between a fellowship in critical care and making sure his toddler survives past age 5.
Latest posts by Adam Thomas (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018
Chris Lipp is one of the founding Fathers for CrackCast. He currently divides his time as an EM Physician in Calgary (SHC/FMC) and in Sports Medicine (Innovative Sport Medicine Calgary). His interests are in paediatrics, endurance sports, exercise as medicine, and wilderness medical education. When he isn’t outdoors with his family, he's brewing a coffee or dreaming up an adventure…..
Latest posts by Chris Lipp (see all)
- CRACKCast E191 – Weapons of Mass Destruction - July 2, 2018
- CRACKCast E189 – Air Medical Transport - June 25, 2018
- CRACKCast E188 – Emergency Medical Service: Overview and Ground Transport - June 21, 2018